
Chiari I (Chiari 1) malformation is the most common variant of the Chiari malformations and is characterised by a caudal descent of the cerebellar tonsils through the foramen magnum. Symptoms are generally proportional to the degree of descent. MRI is the imaging modality of choice. Treatment with posterior decompression is usually reserved for symptomatic patients or those with a syrinx.
On this page:
Epidemiology
Chiari I malformations are more frequently encountered in females 1.
Associations
Although Chiari I malformations are often isolated abnormalities, the following findings may be seen in association:
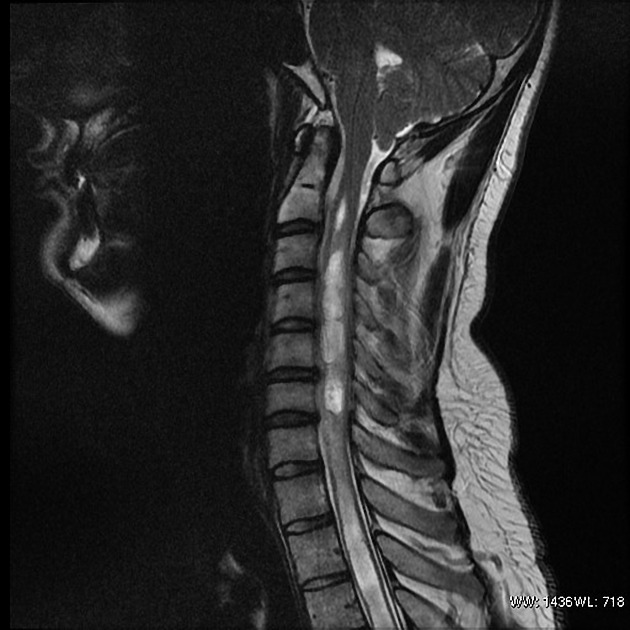
cervical cord syrinx in ~35% (range 20-56%): more common in symptomatic patients
-
hydrocephalus in 7-10% 14 of cases
the relationship remains poorly understood and whether the hydrocephalus or Chiari 1 malformation is the primary abnormality continues to be debated 12
abnormal CSF flow dynamics through the central canal of the cord and around the medulla, posterior fossa size, intracranial pressure and venous pressures have all been implicated as potentially contributory 13
-
skeletal anomalies in ~35% (range 23-45%) 2,3:
Clinical presentation
Unlike Chiari II, III, and IV malformations, Chiari I malformations often remain asymptomatic until adulthood, if it ever becomes symptomatic.
If symptoms are present, they may include a headache and those associated with brainstem compression, syringomyelia, or scoliosis. Headaches are typically located posteriorly and often associated with suboccipital neck pain. Coughing and straining can make the pain worse 15. There are also less defined symptoms which include imbalance, dizziness, cognitive impairment and fatigue 15, which if isolated can be at times difficult to ascribe to tonsillar ectopia, particularly if no other features of CSF flow obstruction is present.
The likelihood of becoming symptomatic is proportional to the degree of descent of the tonsils. In one study, all patients with >12 mm of descent were symptomatic, whereas approximately 30% of those with 5-10 mm descent remained asymptomatic 2 (see MRI section for measurement technique).
Pathology
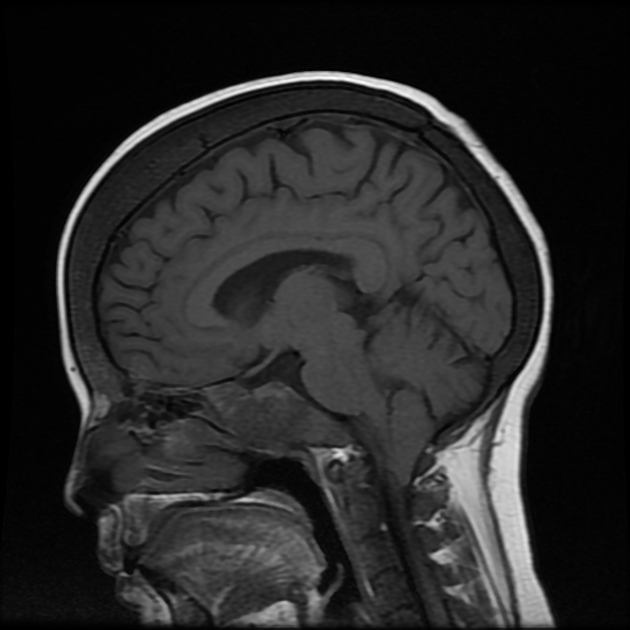
The Chiari I malformation is characterised by an inferior position of the cerebellar tonsils relative to the foramen magnum 16. This is believed to be due to a mismatch between the size and content of the posterior fossa.
Four groups of Chiari I patients can be distinguished, according to different pathogeneses 9:
abnormal skull base (e.g. short clivus)
cervical segmentation anomalies (e.g. Klippel-Feil syndrome)
small cranial vault and/or posterior fossa and consequent overcrowding
excessive brain tissue (sometimes referred to as "acquired Chiari malformation")
Chiari I malformations need to be distinguished from low-lying tonsils (benign tonsillar ectopia) which is an asymptomatic and incidental finding in normal individuals, whereby the tonsils protrude through the foramen magnum by no more than 3-5 mm 1,2. The terminology of caudally displaced tonsils is discussed in the article on cerebellar tonsillar ectopia.
Radiographic features
Although historically visible on myelography, cross-sectional imaging (especially MRI) is needed to diagnose accurately and assess for Chiari I malformations. In either case, the diagnosis is made by measuring the cerebellar tonsillar position (TP).
CT
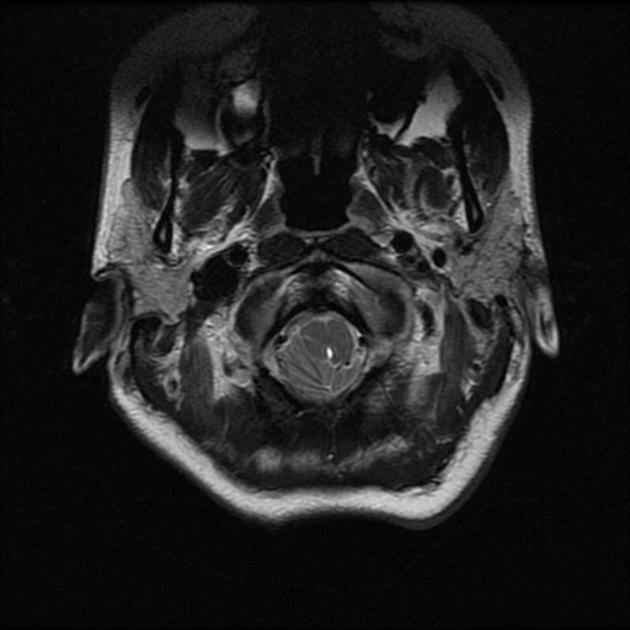
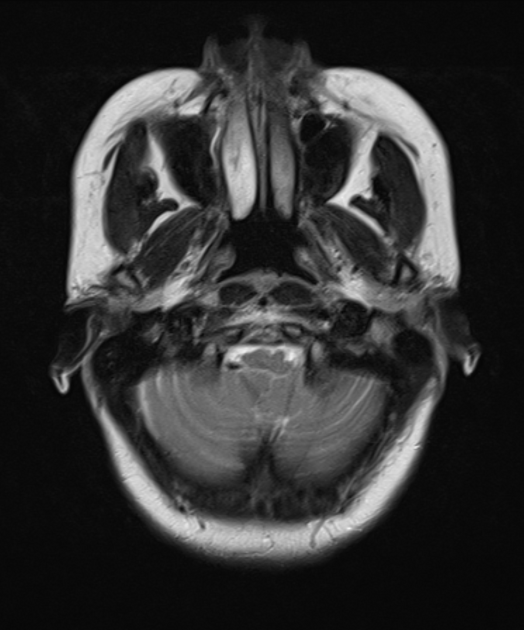
With modern volumetric scanning and high-quality sagittal reformats relatively good views of the foramen magnum and tonsils can be achieved although the intrinsic lack of contrast (compared to MRI) makes accurate assessment difficult. More frequently the diagnosis is suspected on axial images where the medulla is embraced by the tonsils and little if any CSF is present. This is referred to as a crowded foramen magnum.
MRI
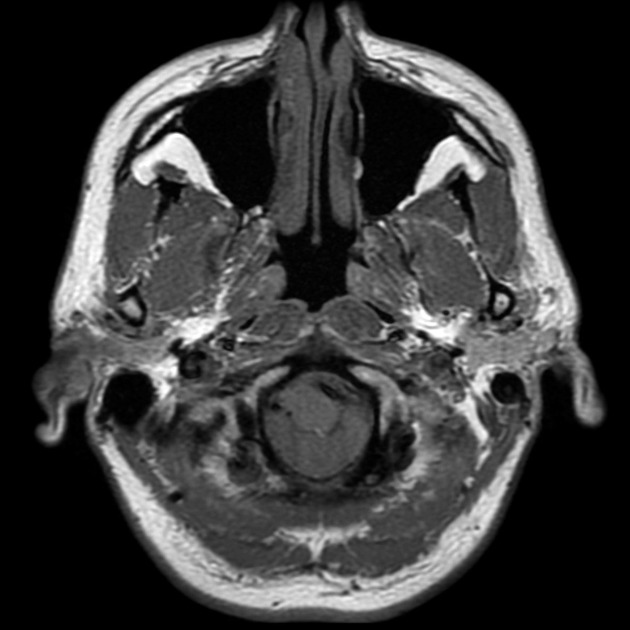
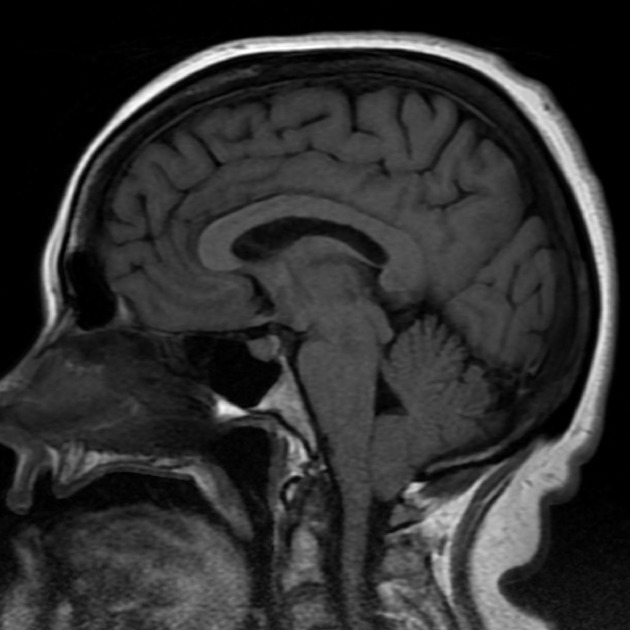
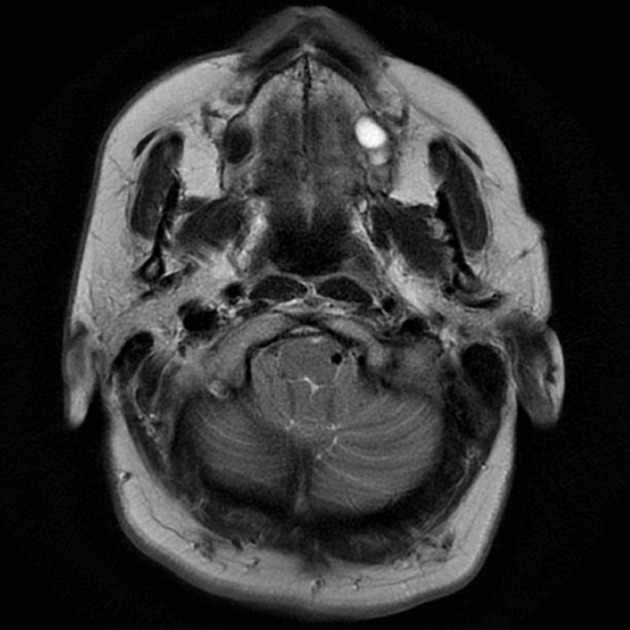
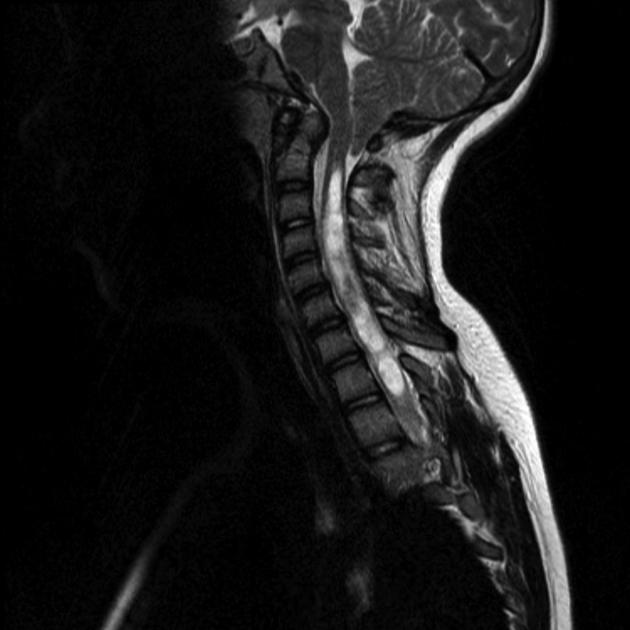
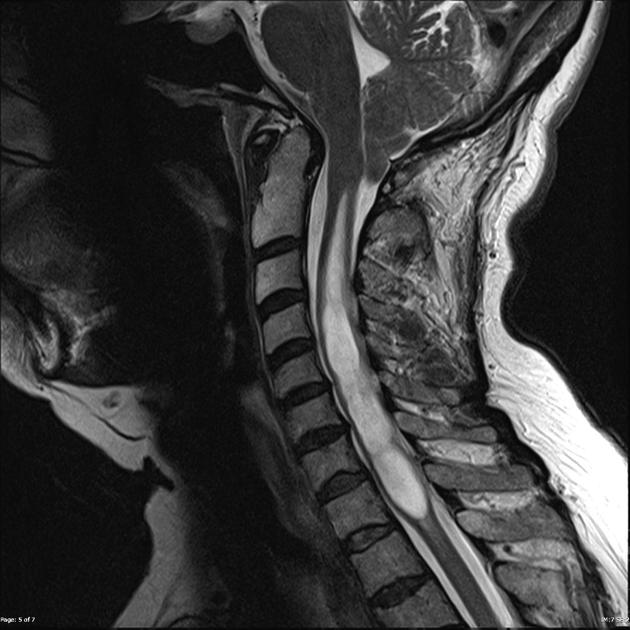
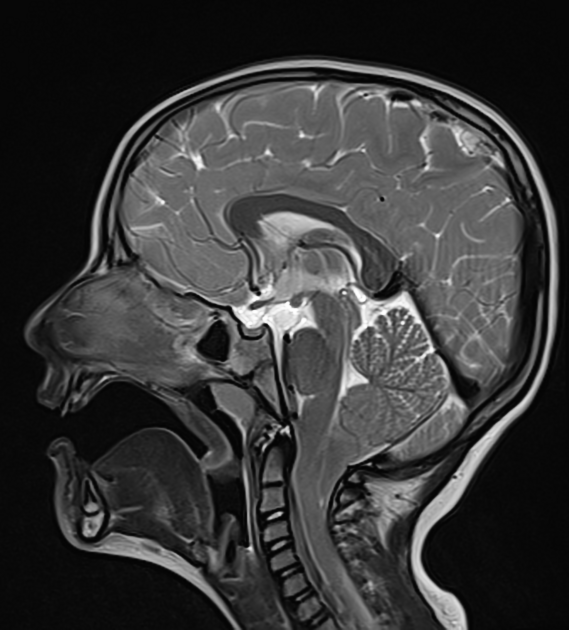
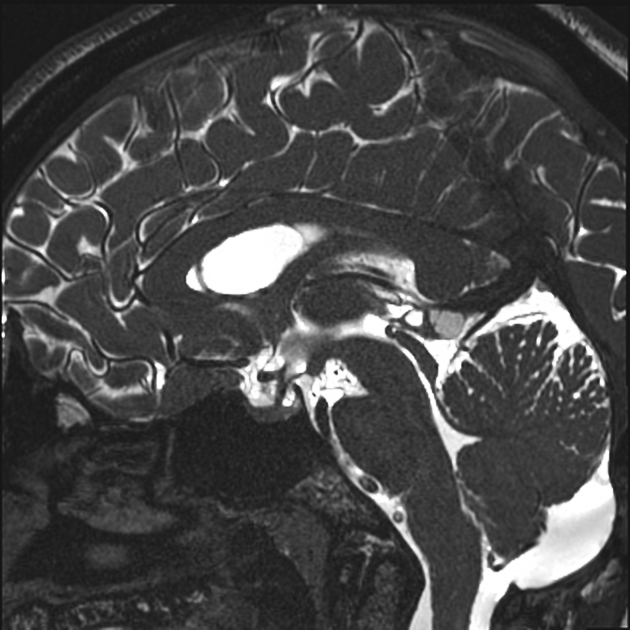
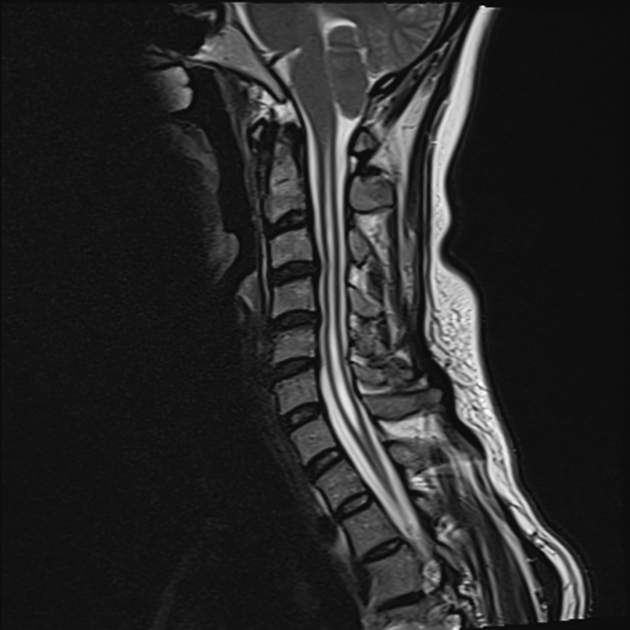
MRI is the imaging modality of choice. On sagittal imaging, the best plane for assessing for the presence of Chiari I malformations, the tonsils are pointed, rather than rounded and referred to as peg-like. The sulci are vertically orientated, forming so-called sergeant stripes. Axial images through the foramen show crowding of the medulla by the tonsils.
Measurement
The degree of tonsillar descent is determined by first drawing a line from the basion to the opisthion (anterior margin to the posterior margin of the foramen magnum); this defines the plane of the foramen magnum.
A measurement is then drawn perpendicular to this plan between it and the tip of the cerebellar tonsils, either in the midsagittal image or an adjacent parasagittal image, wherever the tonsils are most low lying 10,11.
See cerebellar tonsillar position article for more details.
Ancillary features
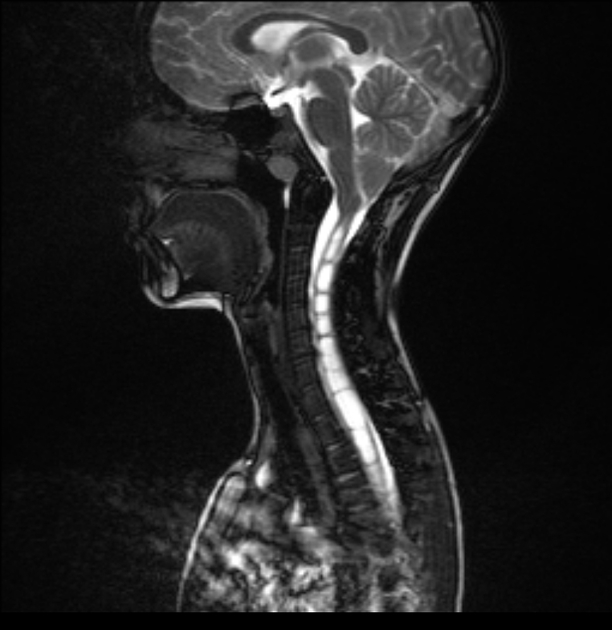
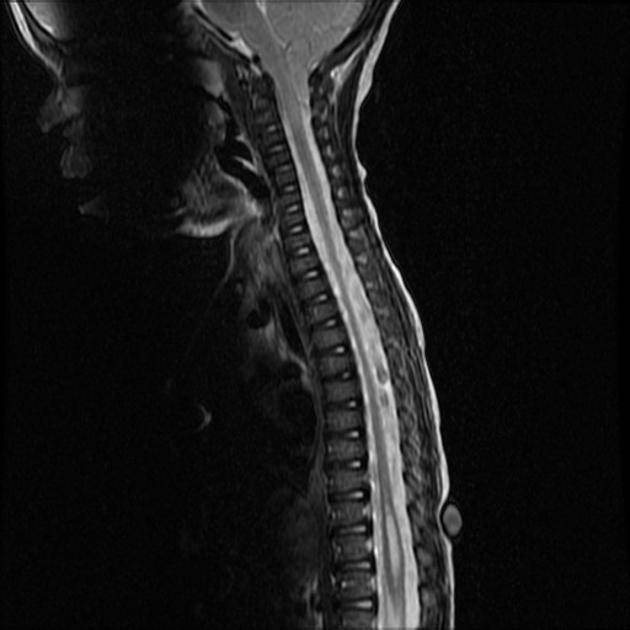
Spinal cord MRI should be recommended as a syrinx may be seen if progressively enlarging or associated with symptoms may be an indication for surgical intervention 5.
CSF flow studies may also be useful to assess the flow surrounding the cervicomedullary junction.
Importantly, features of intracranial hypertension and craniospinal hypotension should be sought to ensure that cerebellar tonsillar ectopia is not secondary to abnormal intracranial pressure (and therefore not a true Chiari I malformation) 7,8.
Treatment and prognosis
Treatment is a surgical posterior fossa decompression and is usually reserved for symptomatic patients (e.g. strain or cough related headaches) or those with a syrinx.
How the posterior fossa decompression is carried out varies but can include a combination of the following: by removing part of the occipital bone and posterior arch of C1, performing a duroplasty, dividing arachnoid adhesions and bands, opening the forth ventricle and resecting part of the tonsils 15.
Successful decompression not only results in symptomatic relief but reduces tonsillar ectopia, reduces the size of the syrinx and restores CSF flow around the cervicomedullary junction 15.
History and etymology
It was first described in 1891 by Hans Chiari (1851-1916), an Austrian pathologist, based on the autopsies of children.
Differential diagnosis
Imaging differential considerations include:
incidental tonsillar ectopia: <5 mm
Chiari 1.5 malformation (sometimes considered a variant of Chiari I malformation 4,16)
-
acquired tonsillar ectopia
Distinguishing Chiari I malformation for pseudotumour cerebri is particularly important as treatment with a posterior fossa decompression can result in poor outcomes 5. Examination for features of intracranial hypertension is therefore crucial.
















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}