
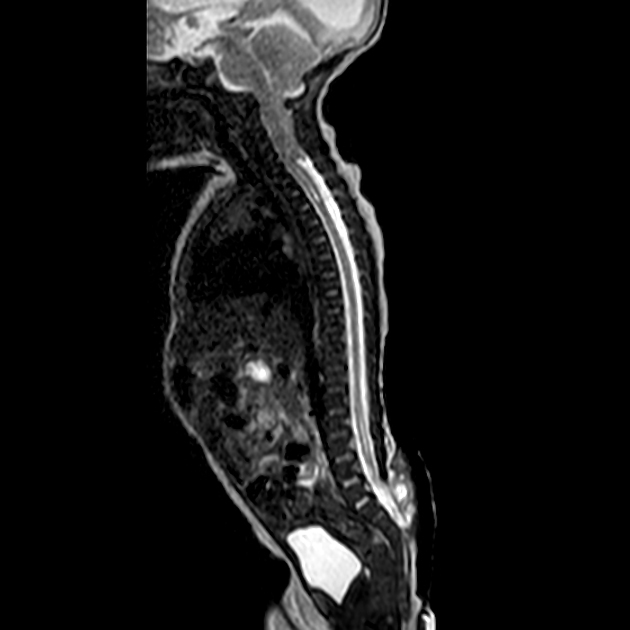
Chiari II (Chiari 2) malformations are relatively common congenital malformations of the spine and posterior fossa characterized by myelomeningocele (lumbosacral spina bifida aperta) and a small posterior fossa with descent of the brainstem, cerebellar tonsils, and vermis through the foramen magnum. Numerous associated abnormalities are also frequently encountered.
On this page:
Terminology
Chiari II malformations are often considered a more severe form of the more common Chiari I malformation. However, it is now understood that these entities are the endpoints of distinct disease processes with some overlapping imaging findings. Chiari III and IV malformations are discussed in their respective articles.
It should be noted that the term Arnold-Chiari malformation should no longer be used; see the Chiari malformations history and etymology section for more information.
Epidemiology
Chiari II malformations are commonly encountered, with an incidence of ~1:1000 live births 7.
When a child is born with a myelomeningocele, the vast majority (~95%) have an associated Chiari II malformation.
Clinical presentation
Given the wide range of anatomical severity, as well as the large number of associated abnormalities that are sometimes encountered, it should be no surprise that the clinical presentation of patients with Chiari II malformations is also varied both in character and severity. The presentation can be divided according to the age of the individual (although most will have lifelong sequelae) as follows 7:
-
neonatal
brainstem dysfunction resulting in cranial nerve palsies
-
child
musculoskeletal
-
young adult
Pathology
While Chiari I malformation is thought to result from a small posterior fossa, Chiari II occurs due to in utero malformation of the spine and cranial structures, resulting in a characteristic displacement of the medulla, fourth ventricle, and cerebellum through the foramen magnum.
As almost all neonatal patients with Chari II have myelomeningocele, it has been suggested that the underlying etiology is that of in utero CSF leak due to open spinal dysraphism. Older patients with Chiari II without myelomeningocele are thought to have had either a smaller neural tube defect or subsequent closure of the defect in utero.
Associations
-
spinal
-
cerebral
fenestration of the falx with interdigitated gyri or absent falx; heart shape incisura
stenogyria/polymicrogyria (probably not the same as polymicrogyria encountered in schizencephaly 7)
-
cranial vault
scalloping of petrous temporal bone 3
Luckenschadel skull
-
skeletal
Radiographic features
Ultrasound
Classical signs described on ultrasound include
There may also be evidence of fetal ventriculomegaly due to obstructive effects as a result of downward cerebellar herniation.
Additionally, many of the associated malformations (e.g. corpus callosal dysgenesis) may be identified.
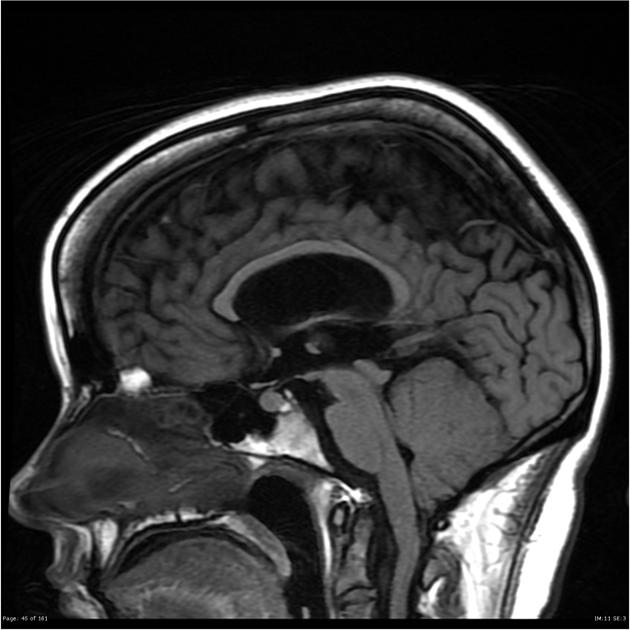
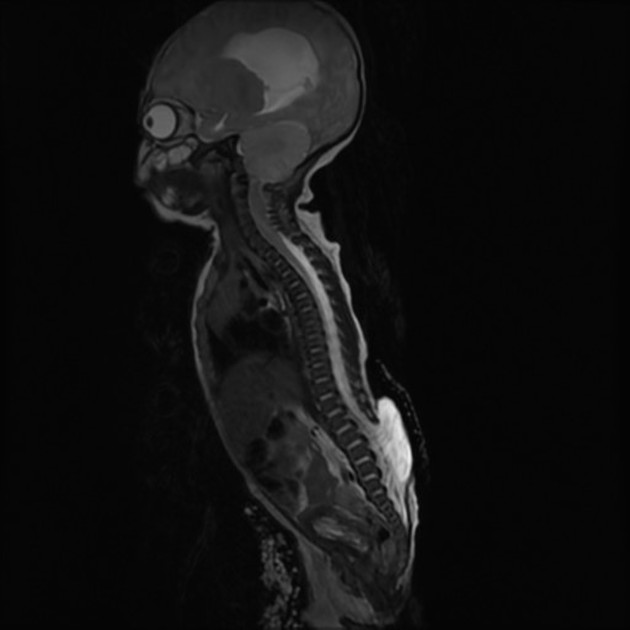
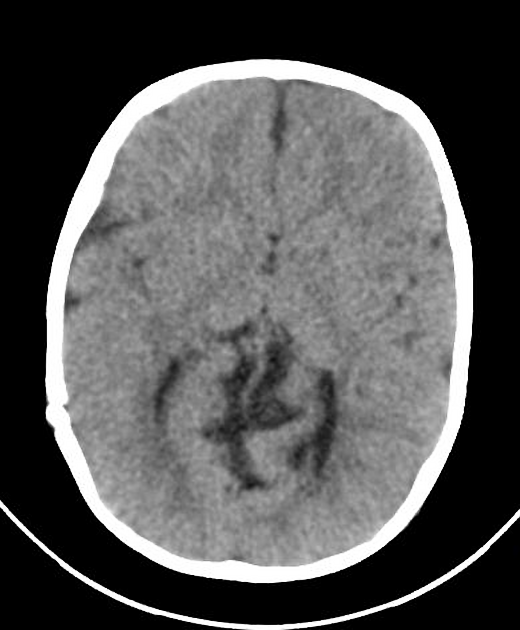
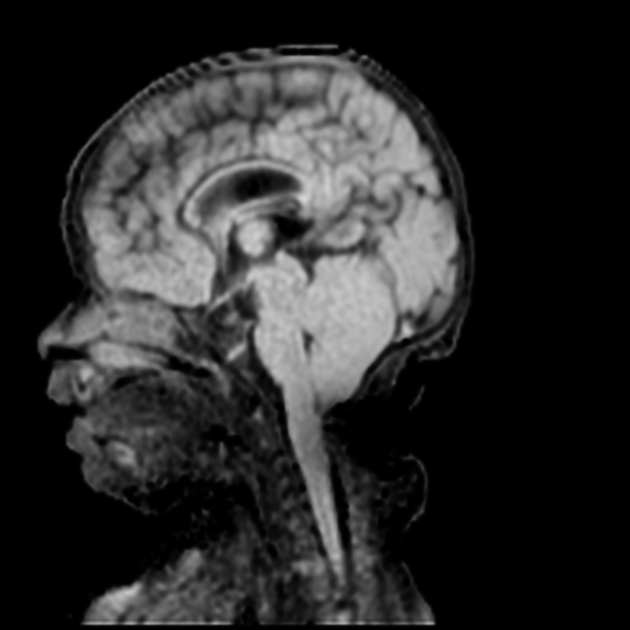
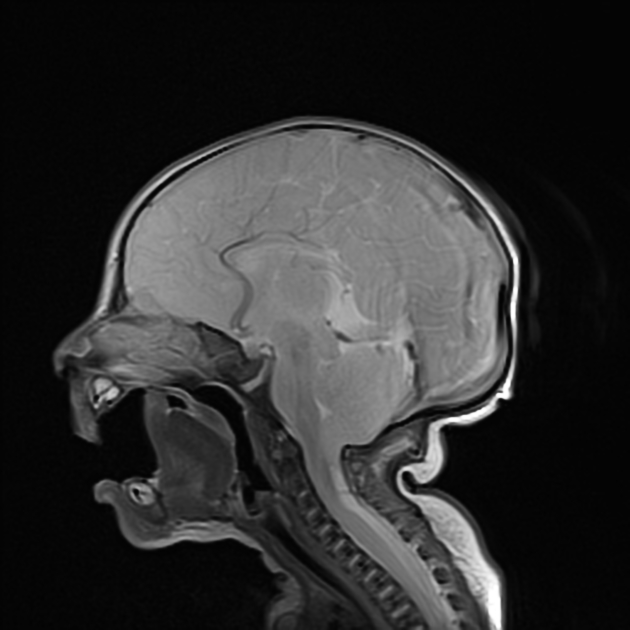
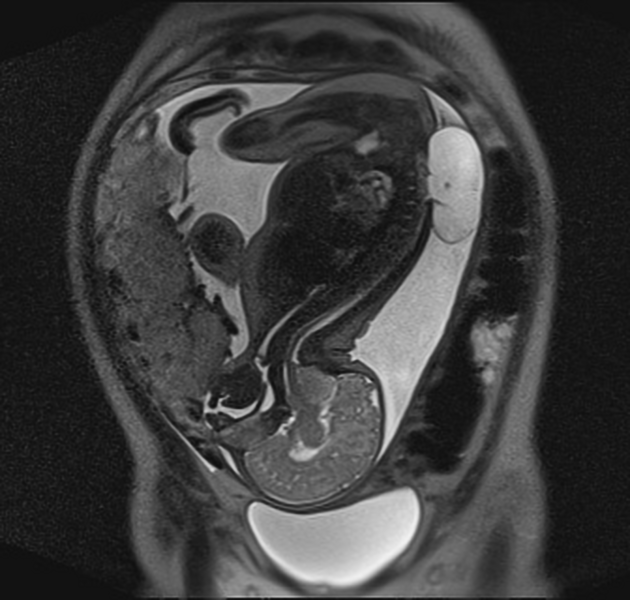
MRI
MRI is the modality of choice for detecting and characterizing the full constellation of findings associated with Chiari II malformations.
The key features are discussed below, whereas the wide range of associated abnormalities (see above) are discussed separately.
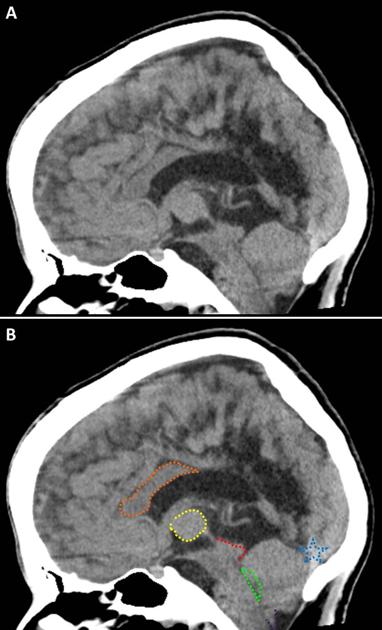
Posterior fossa
small posterior fossa with a low attachment of the tentorium cerebelli and a low torcula
the brainstem appears 'pulled' down with an elongated and low-lying fourth ventricle
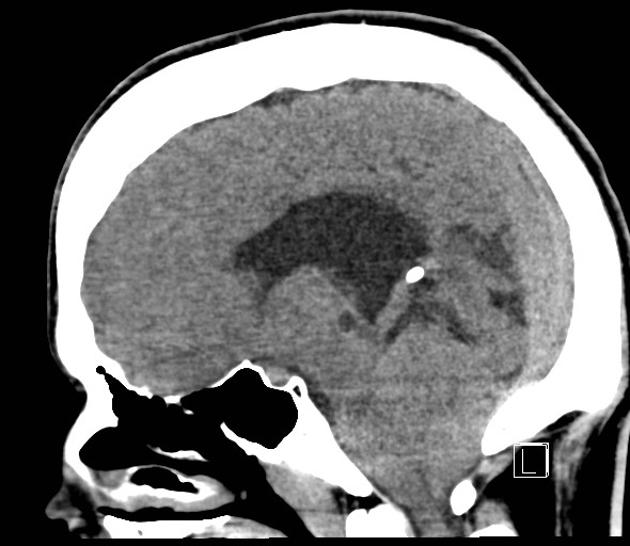
the tectal plate appears beaked: the inferior colliculus is elongated and points posteriorly, with resulting angulation of the aqueduct which results in aqueductal stenosis and hydrocephalus
the cerebellar tonsils and vermis are displaced inferiorly through the foramen magnum, which appears crowded
Spine
Treatment and prognosis
Treatment of patients with Chiari II malformation is complex due to the variable form and severity of malformations:
-
myelomeningocele repair and management of neurogenic bladder
performed on the in utero fetus at some centers in select cases to improve outcomes 9
-
ventricular shunting (usually ventriculoperitoneal)
hydrocephalus usually requires shunting, which can help ameliorate cranial nerve and brainstem dysfunction
-
craniovertebral decompression
may also be required in neonates with brainstem dysfunction if hydrocephalus is not present or symptoms and signs do not improve with shunting
older patients with hindbrain herniation or syringohydromyelia may also benefit
History and etymology
The Chiari malformations were first described in 1891 by Hans Chiari, Austrian pathologist (1851-1916). See the article on Chiari malformations for further details.
Differential diagnosis
The differential is predominantly one of definition, and the term Chiari type II is often inappropriately used to designate a variety of malformations. Provided both myelomeningocele and brainstem descent are present, the diagnosis is usually straightforward 7:
-
does not have a myelomeningocele
may occasionally have brainstem descent
isolated myelomeningocele without posterior fossa abnormality











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.