
Facial nerve schwannoma, also known as facial nerve neuroma/neurilemoma, is a schwannoma that arises from the facial nerve. They are generally uncommon, and when involving the temporal bone, make up less than 1% of all temporal bone tumors.
On this page:
Epidemiology
Facial nerve schwannoma is a rare tumor 2.
Clinical presentation
They can present with a wide variety of symptoms. More frequently they present with gradual, and often incomplete, facial nerve palsy. A rapid onset which mimics Bell palsy is certainly recognized.
Mass effect on adjacent nerves may well cause sensory neural hearing loss (SNHL) or even conductive hearing loss if growth into the middle ear impairs the normal function of the ossicles. In a minority of cases (~10%) the tumor is extra-cranial, where it presents as an asymptomatic parotid mass.
Pathology
As with schwannomas elsewhere, they originate from the surface of the nerve, and displace and splay the nerve fibers over their eccentric growth (this compares favourably to neurofibromas through which the axons are distributed). This allows for potential resection of the tumor while sparing the nerve.
Similar to vestibular schwannomas, they may grow to a quite sizable extent and exert positive mass effect with growth into the cerebellopontine angle.
Location
They can occur in any segment of the facial nerve and have a tendency to involve multiple segments. There is a predilection for the region of the geniculate ganglion.
Radiographic features
Imaging characteristics of the tumor itself are the same as that of schwannomas elsewhere: homogeneous enhancement on both CT and MRI when small; heterogeneous when large. The best clue that a schwannoma is of the facial nerve rather than the more common vestibulocochlear nerve (CN VIII) is expansion extending along the facial nerve canal - especially along the labyrinthine segment.
CT
In all cases, high-resolution thin-section bone CT of the temporal bone is required to assess the otic capsule. Bony scalloping and remodeling may be present. Failure to preoperatively diagnose bony erosion can lead to postoperative fistula formation.
MRI
Signal characteristics include 2
- T1: typically iso- to hypointense relative to grey matter
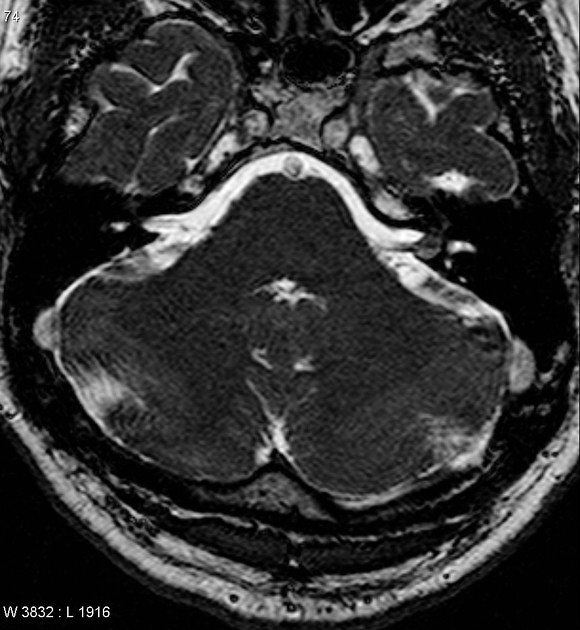
- T2: typically hyperintense; large lesion may show heterogeneous signal
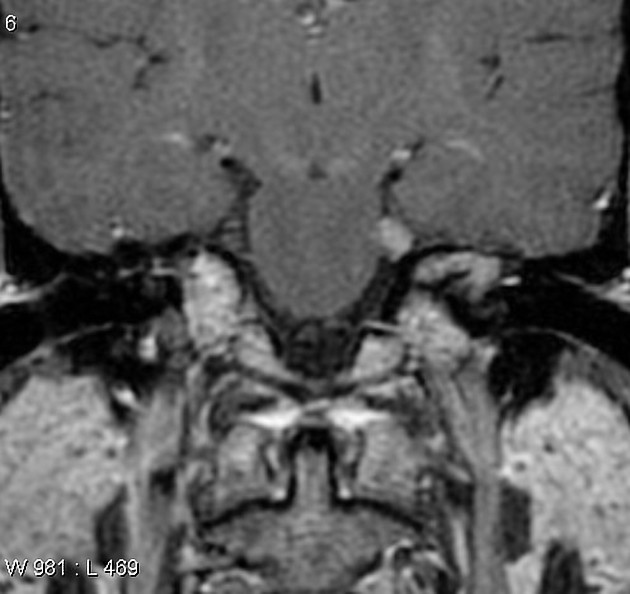
- T1 C+ (Gd): usually demonstrate homogeneous enhancement with larger lesions with cystic degeneration seen as focal intramural low signal intensity
Treatment and prognosis
Management options include nerve resection or tumor debulking, decompression of the facial nerve canal, radiosurgery, and observation 4. The choice depends on the level of residual facial nerve function, hearing function, comorbidities, and patient preference 4.
Differential diagnosis
The differential depends on location of the lesion:
- when in an intraparotid location, consider the differential for a parotid mass
- when in the temporal bone, consider the differential for middle ear tumors
- when at the cerebellopontine angle and internal auditory canal, consider the differential for cerebellopontine angle mass






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.