
Gastric volvulus is a specific type of volvulus that occurs when the stomach twists on its mesentery. It should be at least 180° and cause bowel obstruction to be called gastric volvulus. Merely gastric rotation on its root is not considered gastric volvulus.
On this page:
Epidemiology
Organo-axial volvulus is more common in adults, responsible for 60% of presentations. Mesentero-axial volvulus is more common in children.
Clinical presentation
Patients may present with the classic triad of Borchardt:
severe sudden epigastric pain
intractable retching without vomiting
inability to pass a nasogastric tube
Chronic symptoms are more common in patients with mesentero-axial volvulus.
Pathology
Subtypes
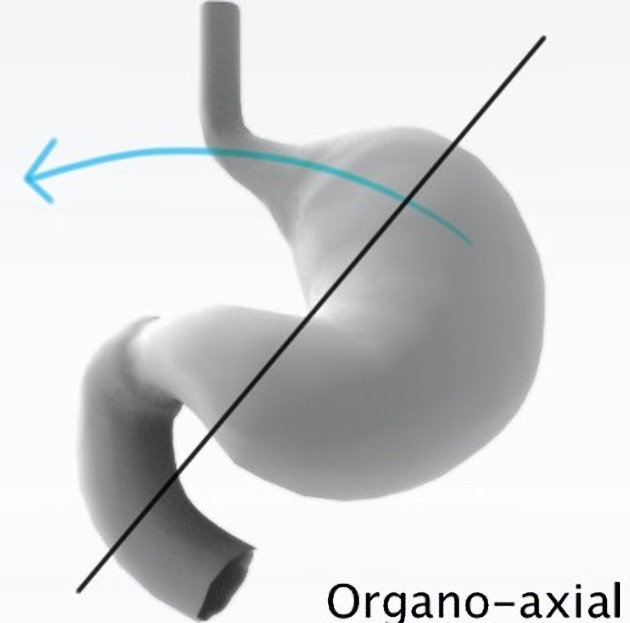
Organo-axial volvulus
more common of the two types in adults (2/3 of cases)
commonly occurs in the setting of trauma or para-esophageal hernia
stomach is rotated along its long axis (along the cardiopyloric line, which is drawn between the cardia and the pylorus)
-
mirror image of normal anatomy can occur with reversal of the greater and lesser curves
antrum rotates anterosuperiorly
fundus rotates posteroinferiorly
complete (>180º) present with obstruction or ischemia
incomplete rotation (<180º), also called organo-axial position of the stomach, usually asymptomatic
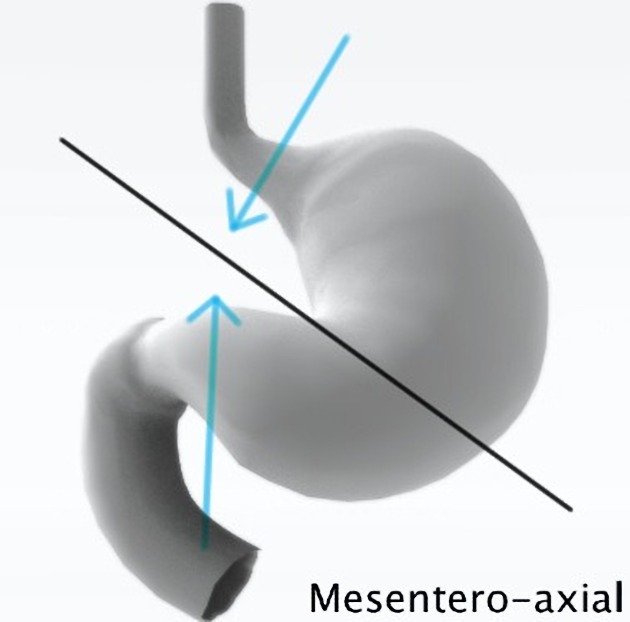
Mesentero-axial volvulus
less common in adults, but is more common than organo-axial volvulus in the pediatric population (59% of gastric volvulus)
-
rotation around short axis from the lesser to greater curvature (i.e. perpendicular to the cardiopyloric line)
usually incomplete, <180°
displacement of antrum above gastro-esophageal junction; stomach appears upside-down with the antrum and pylorus superior to the fundus and proximal body
coincides with the axis of mesenteric attachment and is associated with severe obstruction and strangulation
less associated with diaphragmatic defect
plain films may show an intrathoracic stomach with two air fluid levels 1
Associations
Radiographic features
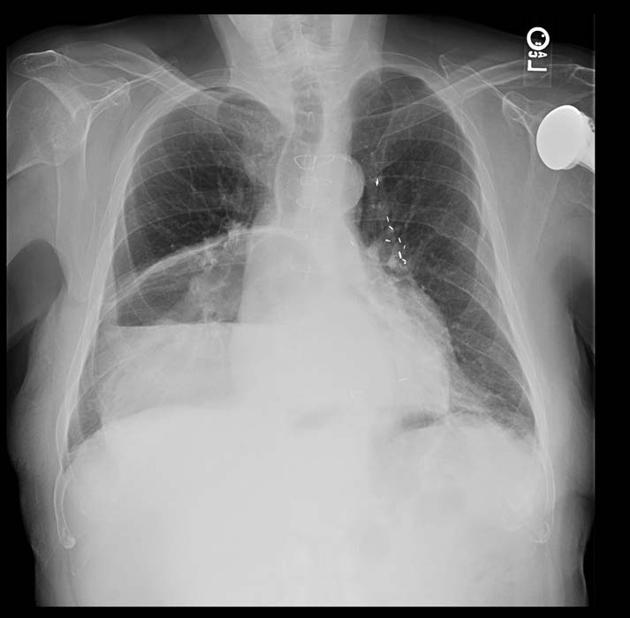
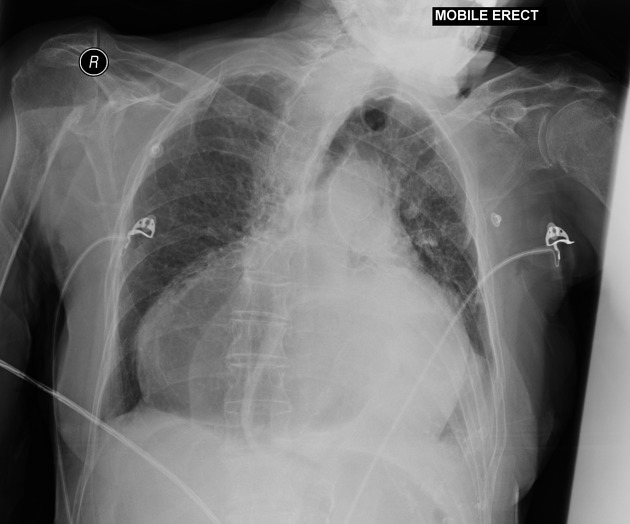
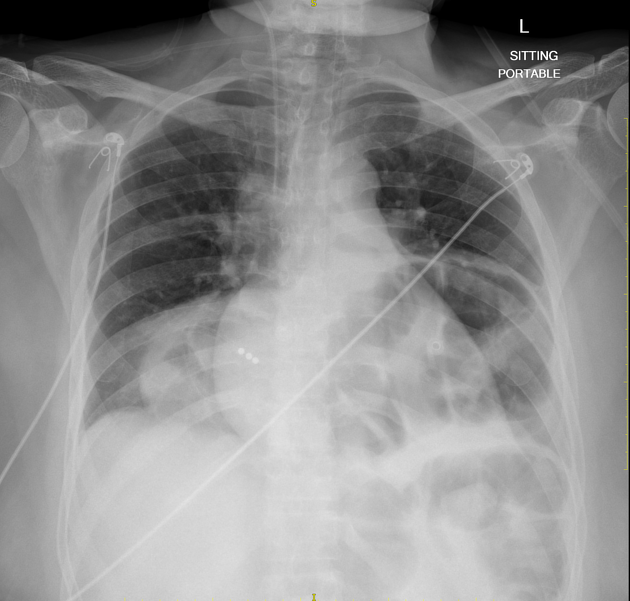
Plain radiograph
-
chest radiograph
-
intrathoracic; upside-down stomach
mediastinal or retrocardiac air-fluid level
-
-
abdominal radiograph; when performed with the patient upright
unexpected location of the gastric bubble
double air-fluid level
large, distended stomach
collapsed small bowel
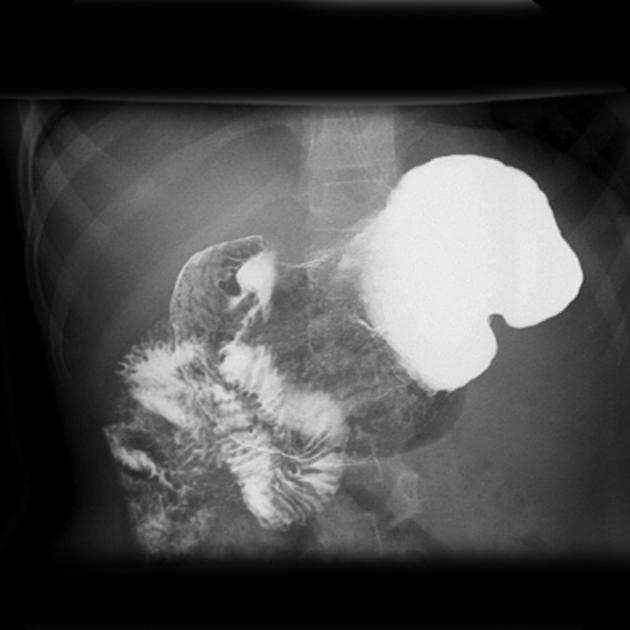
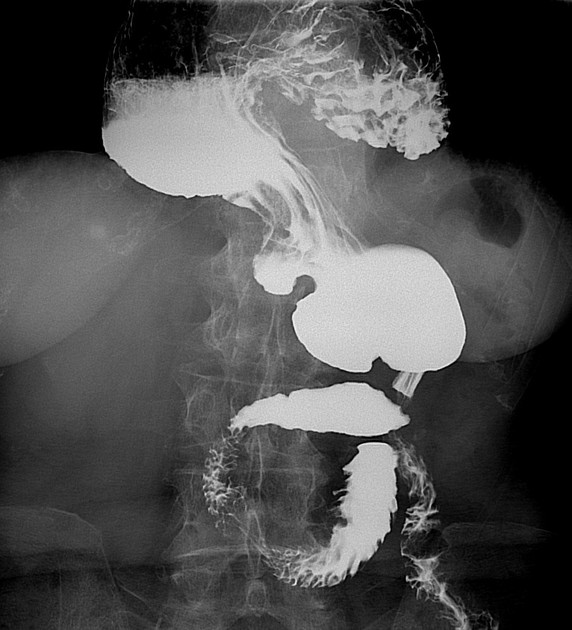
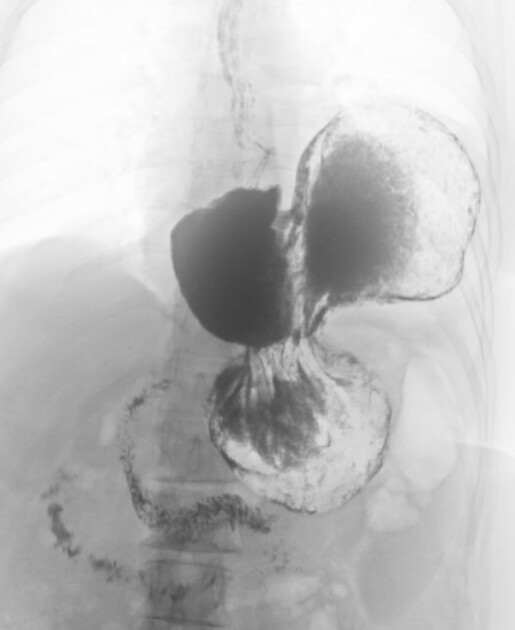
Fluoroscopy
Upper GI
distended stomach in left upper quadrant extending into thorax
inversion of stomach
volvulus with >180° twist causes luminal obstruction
incomplete or absent entrance of contrast material into and/or out of stomach is indicative of acute obstructive volvulus
"beaking" may be demonstrated at point of twist
mesenteroaxial: antrum and pylorus lie above gastric fundus
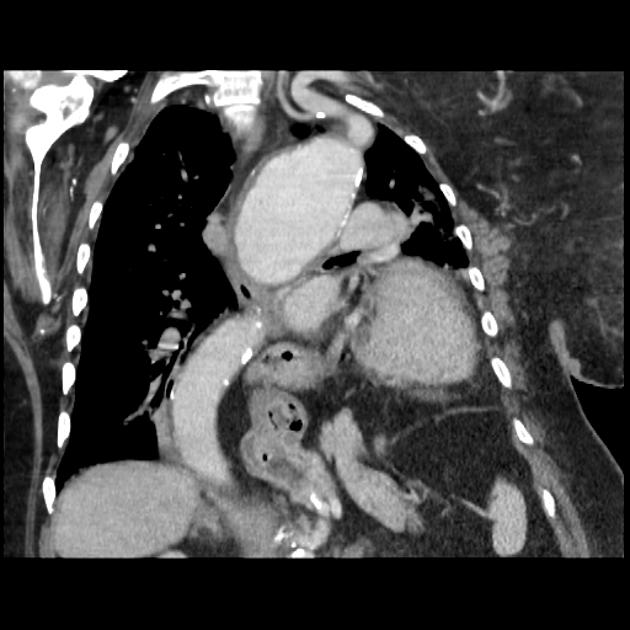
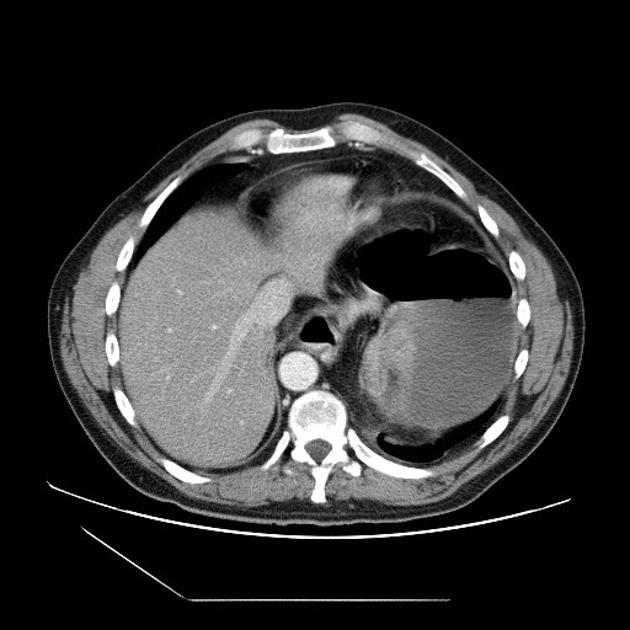
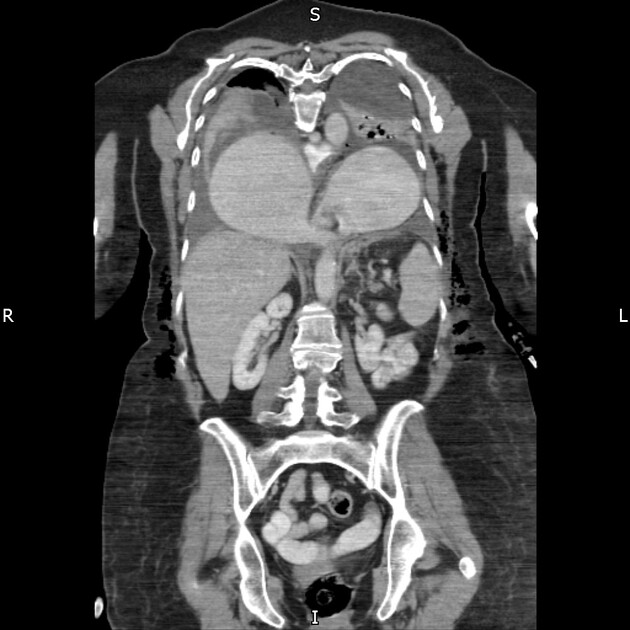
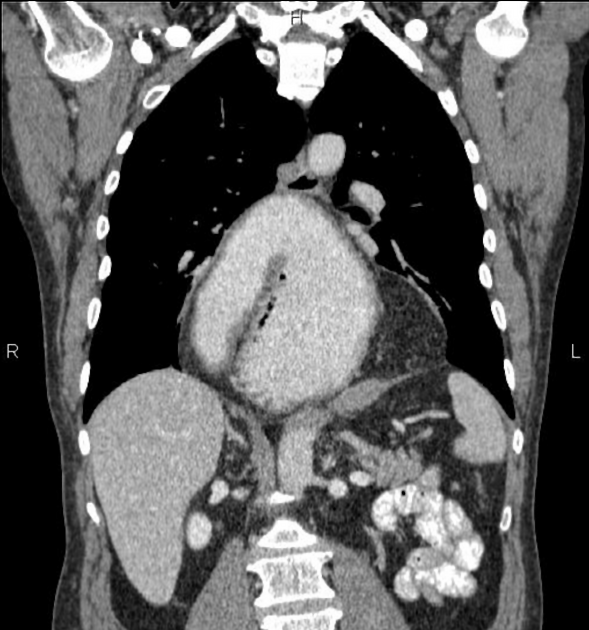
CT
The appearance depends on points of torsion, extent of gastric herniation, and final positioning of stomach:
distended stomach with antropyloric transition point, located at the level of or superior to the fundus 9
linear septum may be visible within the gastric lumen which corresponds to the site of torsion
-
entire stomach may be herniated (type IV paraesophageal hernia (PEH)) or only part of it (type III PEH)
-
both can result in
volvulus
obstruction
ischemia
ischemia seen as lack of contrast enhancement of gastric wall, with or without pneumatosis
-
Treatment and prognosis
Surgical repair, including stomach detorsion and gastropexy, is the main treatment modality for gastric volvulus. Detorsion may be performed open or laparoscopically. If the stomach is strangulated or necrotic, gastric resection may be required.
Differential diagnosis
paraesophageal hernia with incarceration of the gastric antrum and duodenal bulb
postoperative state of the stomach












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.