
Intraosseous ganglion cysts, intraosseous ganglia or juxta-articular bone cysts are benign tumor-like non-neoplastic lesions occurring in the subchondral regions of bone in the absence of degenerative or inflammatory arthritis 1,2.
On this page:
Epidemiology
Intraosseous ganglion cysts tend to occur in middle age with a peak incidence in the 4th and 5th decade of life 1-4 and seem to be slightly more common in men 1,3.
Diagnosis
The diagnosis of intraosseous ganglia is usually made by a combination of clinical history/examination and typical imaging characteristics. If they are excised the diagnosis can be confirmed histologically.
Clinical presentation
Patients might present with localized pain, swelling and/or tenderness 1-4 or might be asymptomatic 1.
Complications
A potential complication of an intraosseous ganglion cyst is a pathological fracture 2.
Pathology
They are uni-/multilocular cysts within bone adjacent to joints. They contain mucoid viscous gelatinous material and are surrounded by a fibrous lining. Unlike subchondral cysts they do not have an epithelial or synovial lining 2. Most intraosseous ganglia are small (up to 1-2 cm) and larger lesions of >5 cm are rare 2.
Etiology
Possible theories on the pathogenesis are 1-3:
mucoid degeneration of intraosseous connective tissue due to altered mechanical stress
occasional penetration of juxta-osseous soft-tissue ganglion into the underlying bone
However, the exact etiology is unknown 1,2.
Location
Common locations are 1-4:
epiphyses and metaphyses of long bones (tibia, femur, humerus, ulna)
Radiographic features
Intraosseous ganglia are cystic well-defined lesions located close to joints, they have similar imaging features as subchondral cysts except that there are no degenerative changes of the joint. They might show signs of cortical expansion/thinning and an articular (i.e. communicating ganglion cyst) or non-articular cortical defect is common 1,9. Periosteal reaction should be absent 9.
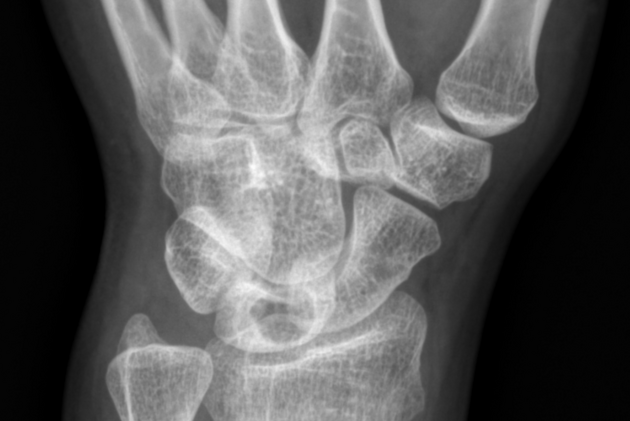
Plain radiograph
A solitary well-defined lytic lesion in a subchondral region with a sclerotic margin 1-4.
CT
On CT intraosseous ganglia appear as solitary lucent bone lesions with sclerotic inner margin 9 near joints.
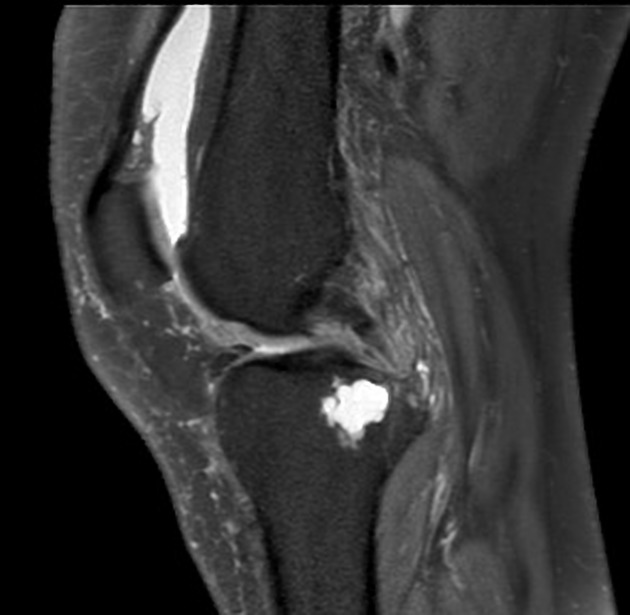
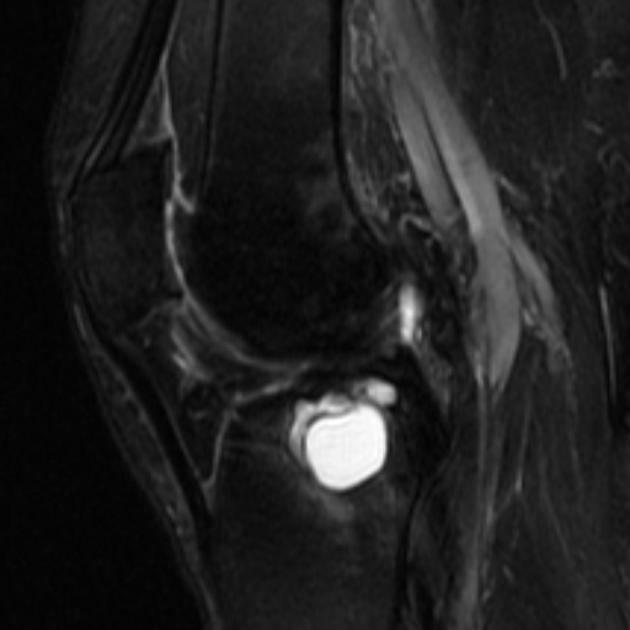
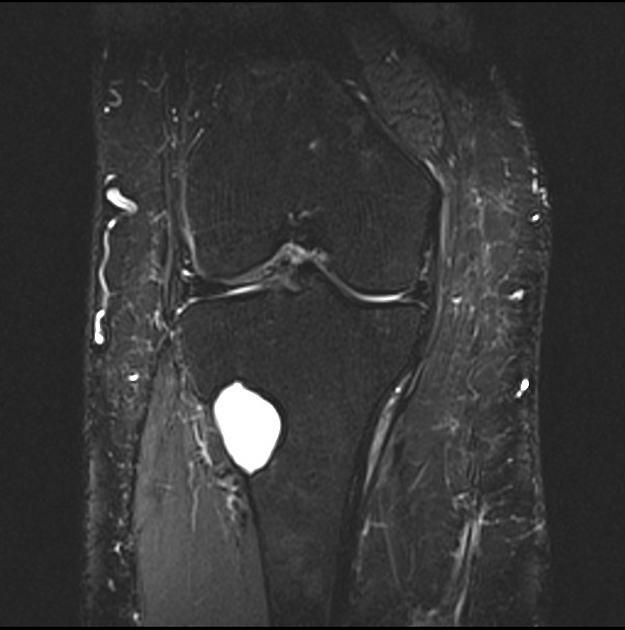
MRI
Intraosseous ganglia appear as solitary, unilocular or multilocular 5 lesions and are usually homogeneous with a sclerotic rim 9. Fluid-fluid levels can be rarely seen 9. Bone marrow edema adjacent to the ganglion cyst is also common 9.
Signal characteristics
T1: isointense-to-high signal (compared to skeletal muscle)
T2/STIR: high signal
T1C+: rim enhancement more common than heterogeneous enhancement 9
Nuclear medicine
Bone scintigraphy demonstrates increased radiotracer uptake 9.
Treatment and prognosis
The management will depend on the size and clinical presentation. Small asymptomatic intraosseous ganglion cysts will not need any treatment, whereas symptomatic intraosseous ganglion cysts are probably treated by surgical excision with curettage and subsequent bone grafting 2,3. Recurrences have been reported 1.
History and etymology
An intraosseous ganglion was described by Geoffrey R Fisk in 1949 6.
Differential diagnosis
Imaging differentials include the following 1-4:
subchondral cyst: adjacent degenerative joint disease present otherwise indistinguishable on imaging 9



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.