
Kartagener syndrome (also known as Kartagener-Afzelius syndrome) describes a phenotypic triad which applies to the 50% of primary ciliary dyskinesia which include situs inversus as a feature.
On this page:
Epidemiology
The prevalence of primary ciliary dyskinesia is approximately 1 in 12,000-60,000 5. Situs is random, and approximately 50% of patients with primary ciliary dyskinesia have situs inversus. There is no gender predilection.
Clinical presentation
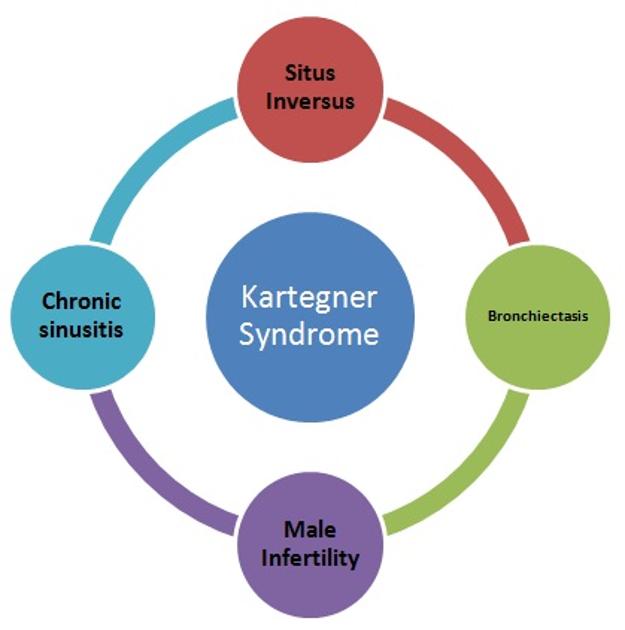
Kartagener syndrome is characterized by the clinical triad of 1:
Other features include:
telecanthus: widened distance between the medial canthi by a nasal polyp
infertility in males
subfertility in females
Radiographic features
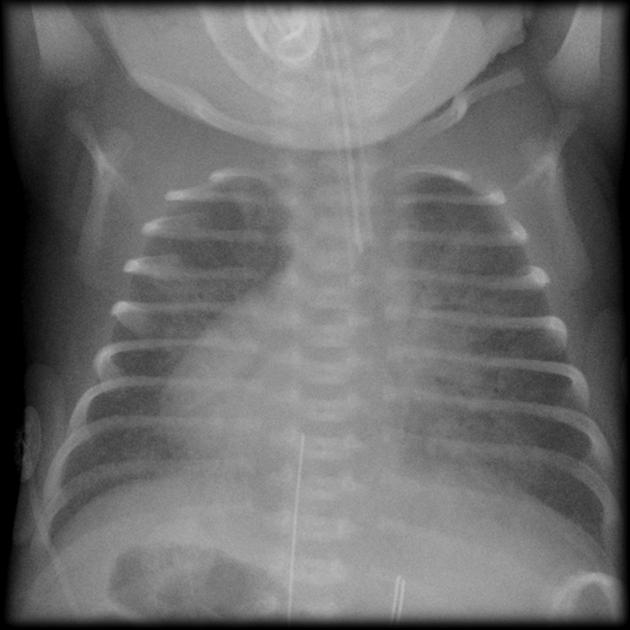
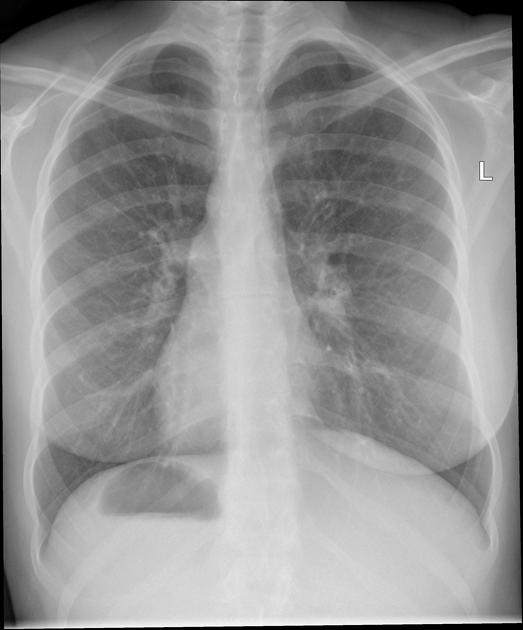
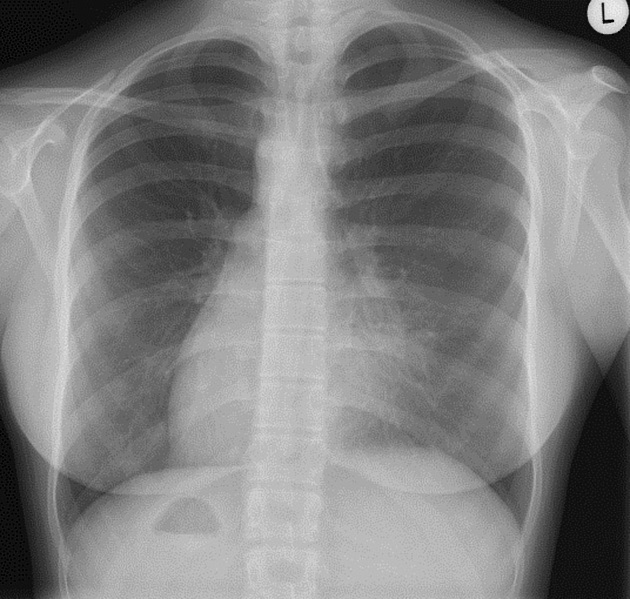
Plain radiograph
Chest radiographic findings depend on the severity of underlying bronchiectasis. Findings may include bronchial wall thickening and bronchial dilatation with the loss of normal peripheral tapering:
predilection to involve the right middle, lingular segment of the left upper lobe and the lower lobes
mucus plugs may be visible (finger in glove sign)
consolidation
situs abnormality, i.e. situs inversus
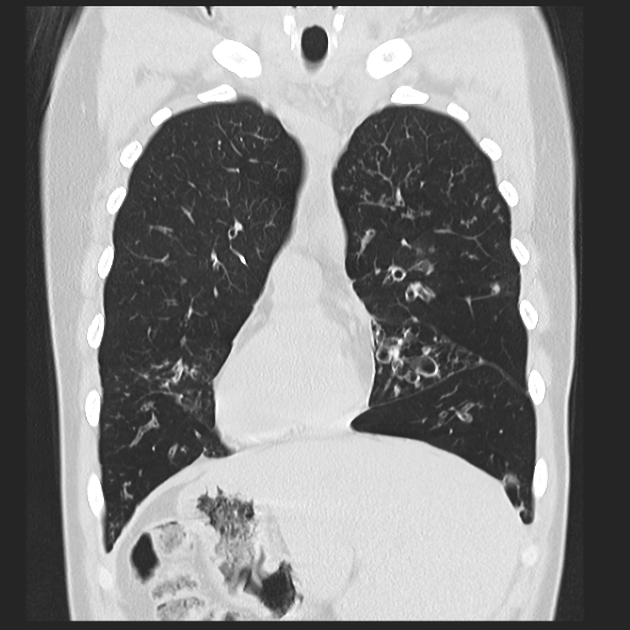
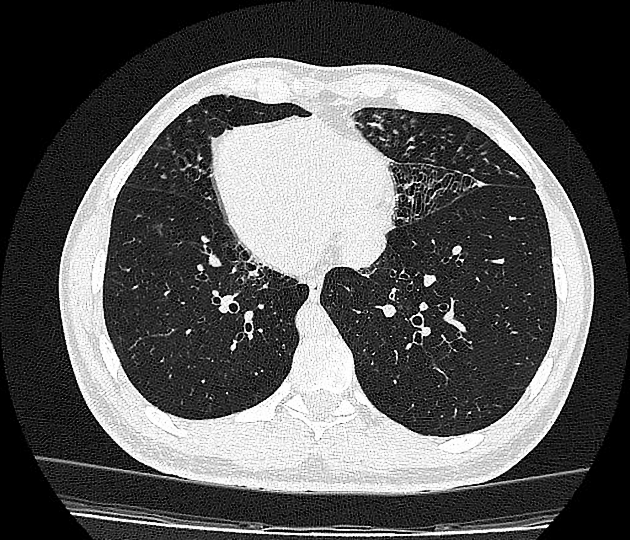
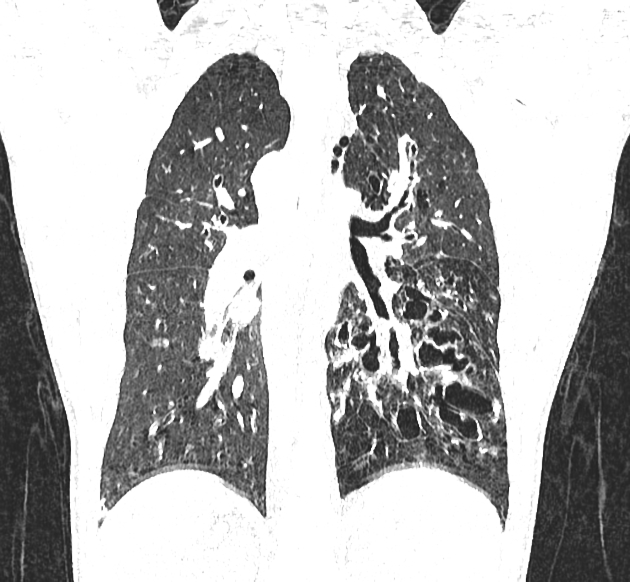
CT
CT tends to demonstrate bronchiectasis which may be variable in severity. However, changes are much milder than in cystic fibrosis 4. The morphology of bronchiectasis can be tubular/cylindrical or saccular/cystic. Also, CT demonstrates:
mucocele, impacted mucus in bronchioles
-
tree-in-bud pattern or centrilobular nodules
may be encountered with mucus impaction and endobronchial spread of infection
mosaic perfusion/air trapping as ancillary findings
eventual scarring may result from recurrent infection, requiring pulmonary resection surgery
bronchial arterial enlargement may be seen
Differential diagnosis
Situs abnormality in association with lower lobe bronchiectasis should prompt the diagnosis of Kartagener syndrome.
For other causes of lower lobe bronchiectasis which are independent of a situs abnormality, see page on lower lobe bronchiectasis.
History and etymology
Manes Kartagener (1897-1975) was a Zurich pulmonologist who first reported the clinical triad of sinusitis, bronchiectasis, and situs inversus in 1933 3,7. He was unaware of male infertility being part of the phenotype of the disease 8.
In the 1970s, Bjorn Afzelius (d. 2008) 9 a cell biologist with an interest in electron microscopy, noted the diversity of structural defects which can affect the dynein arms and/or radial spokes of the tail of immotile sperm 3. While investigating rare cases of men with immotile spermatozoa, he noted a frequency of situs inversus and dysfunction of other ciliated organs 8. It was Afzelius who made the connection with the syndrome previously described by Kartagener. The importance of Afzelius's work is the reason that some now call the eponymous condition, Kartagener-Afzelius syndrome 10.
In 1975, soon after his discovery Bjorn Afzelius wrote to Manes Kartagener with the news. Sadly he received a reply from Kartagener's daughter that he had died several weeks earlier, in August 1975 9.
Further work was undertaken by Jennifer Sturgess, an ultrastructuralist from Toronto, who identified the radial spoke defect as a common feature of Kartagener syndrome and immotile cilia syndrome. She also contributed to research in cystic fibrosis, which shares clinical similarity to primary ciliary dyskinesia.








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.