
Meconium peritonitis refers to a sterile chemical peritonitis due to intrauterine bowel perforation and spillage of fetal meconium into the fetal peritoneal cavity. It is a common cause of peritoneal calcification.
On this page:
Epidemiology
The estimated prevalence is at ~1 in 35,000.
Associations
cystic fibrosis: does not usually calcify in these cases due to lack of enzymes
-
intestinal atresia
Pathology
The etiology is thought to be the result of a sterile chemical reaction resulting from bowel perforation in utero. The bowel perforates as a result of bowel obstruction, such as an atresia or meconium ileus. Secondary inflammatory response results in the production of fluid (ascites), fibrosis, calcification and sometimes cyst formation. Usually, the perforation seals off and the bowel is intact at birth. Intra-peritoneal meconium usually calcifies, sometimes within 24 hours.
Classification
At least four types are recognized:
fibro-adhesive (dense mass: the intense chemical reaction causes the formation of a dense mass with calcium deposits that eventually seal off the perforation)
cystic
generalized
healed
Radiographic features
Plain radiograph
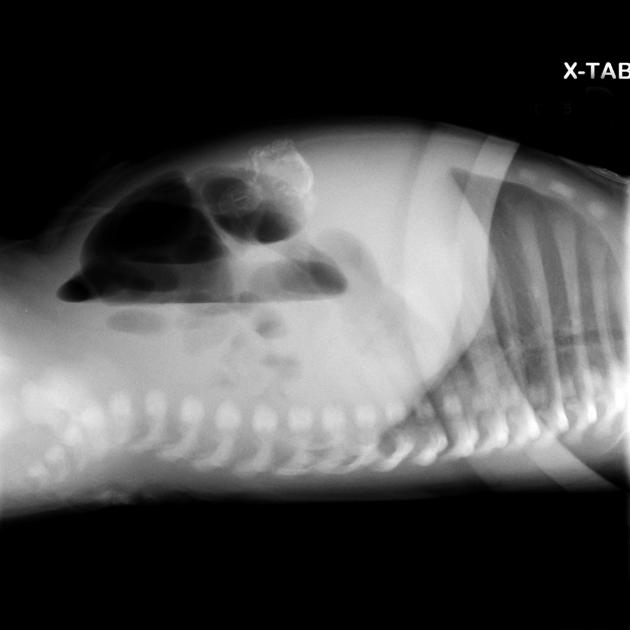
Abdominal radiographs may show:
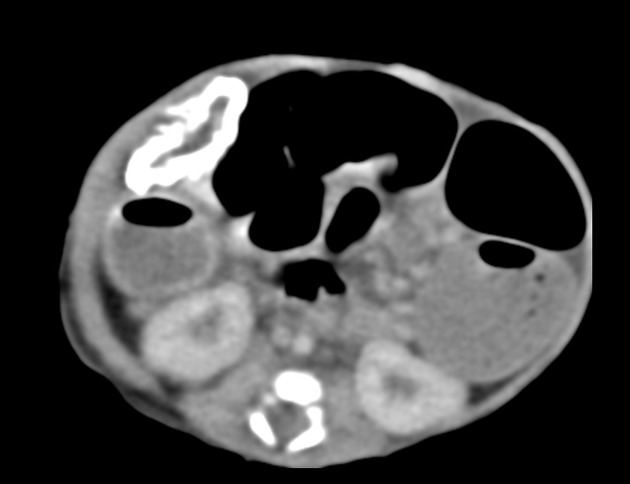
intra-abdominal (peritoneal) calcification (can be curvilinear, linear or flocculant)
a mass containing calcification in the context of a meconium pseudocyst
if the processus vaginalis is patent at the time of perforation, calcification may also be seen in the scrotum
Ultrasound
may show highly echogenic linear or clumped foci which represent calcification 3-4
can also give a snowstorm appearance 4
differentiated from other causes of intra-uterine calcification by its peritoneal distribution
may show fetal ascites (most common antenatal sonographic finding 6) and/or polyhydramnios 11
the abdominal circumference may be increased
may also show associated anomalies such as dilated fetal bowel and/or meconium pseudocysts
may show dilated stomach due to ileus
Treatment and prognosis
When the calcifications are isolated, there generally is a favorable neonatal outcome and intervention is not necessary 11. These cases are thought to represent perforation of bowel that spontaneously heals in utero. Therefore, in the absence of other findings, isolated calcifications can be followed sonographically during pregnancy.
Complications
ascites: tends to be more echogenic than simple ascites 10
bowel obstruction from the formation of fibro-adhesive bands
meconium pseudocyst formation (a walled-off mass of meconium surrounded by a calcific rim)





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.