
Neurofibromatosis type 1 (NF1), also known as von Recklinghausen disease, is a multisystem neurocutaneous disorder, the most common phakomatosis, and a RASopathy. Additionally, it is also one of the most common inherited CNS disorders, autosomal dominant disorders, and inherited tumor syndromes.
Individual systemic manifestations are discussed individually:
The remainder of this article pertains to a general discussion of neurofibromatosis type 1.
On this page:
Epidemiology
Neurofibromatosis affects 1:2500-3000 individuals 3. In half of the cases, the disease is inherited as an autosomal dominant condition. In the other half, the disease is due to a de novo mutation 6. There is a variable expression but 100% penetrance by 5 years of age 6.
Clinical presentation
As is the case with many phakomatoses, NF1 results in a variety of abnormalities of variable severity. To make the clinical diagnosis two or more of the following are required 2:
≥2 neurofibromas or ≥1 plexiform neurofibroma
distinctive osseous lesion (such as sphenoid wing dysplasia or thinning of long bone cortex with or without pseudoarthrosis)
>6 café au lait spots evident during one year (prepubertal >0.5 cm, postpubertal >1.5 cm in size)
axillary or inguinal freckling
≥2 iris hamartomas (Lisch nodules)
a primary relative with NF1
A mnemonic to help remember these features is CAFE SPOT.
In addition, ~45% (range 30-60%) of patients have learning disabilities, and approximately 1% have hypertension due to renal artery stenosis.
It is important to consider that NF1 has a much earlier age of onset than schwannomatosis and NF2, with approximately 50% of patients meeting the diagnostic criteria for NF1 by the age of 1 year and approximately 97% meeting the criteria by the age of 8 years 10.
Neoplasms
It should come as no surprise that a disease due to the inactivation of a tumor suppressor gene (see below) is also associated with an increased incidence of numerous tumors 1-6:
neuroendocrine tumors (NETS)s, such as pheochromocytoma, paraganglioma, and pancreatic NETs 15
malignant peripheral nerve sheath tumor (MPNST) (~10% of patients) 7
-
glioma
juvenile pilocytic astrocytoma (~20% of patients) 13
high grade astrocytoma with piloid features
Pathology
The NF1 gene locus is on chromosome 17q11.2 and the gene product is neurofibromin, which acts as a tumor suppressor of the Ras/MAPK pathway; inactivation of the gene thus predisposes to tumor development 6,12,13. For this reason, the disorder is classified as a RASopathy 12.
The disease primarily is a hamartomatous disorder that involves the ectoderm and mesoderm. Usually, three types of neurofibromas occur in this disorder and are distinguished on the basis of their gross and microscopic appearances.
localized neurofibroma (cutaneous neurofibroma): the most common type, is a focal lesion that typically is located in the dermis and subcutis
diffuse neurofibroma (subcutaneous neurofibroma): localized in the subcutis, usually in the head and neck region
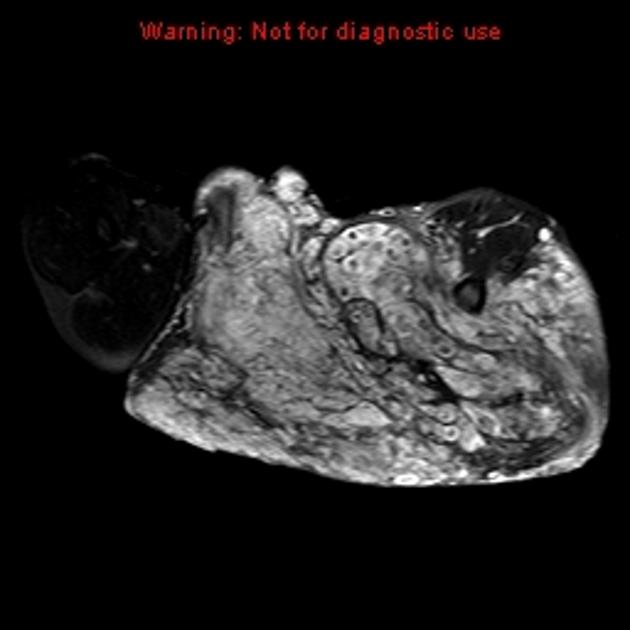
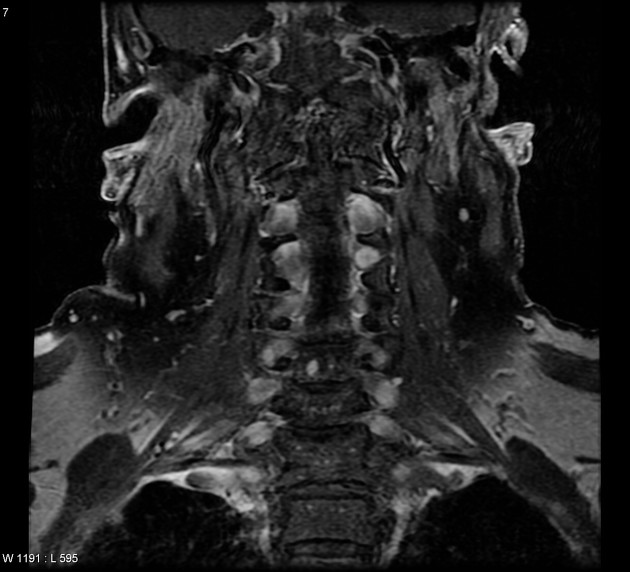
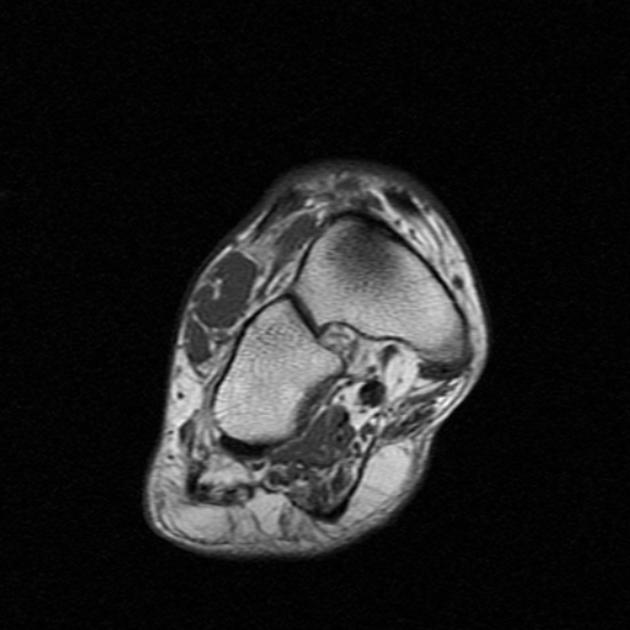
plexiform neurofibroma: considered pathognomonic if present; they may be seen in virtually any location but usually occur in the neck, pelvis, and extremities
Radiographic features
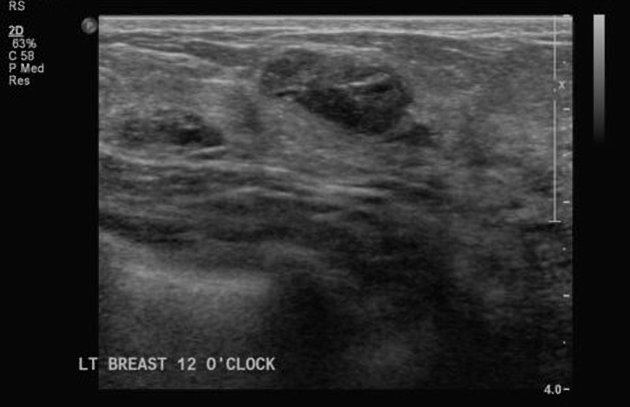
Breast
See breast manifestations of NF1 for details.
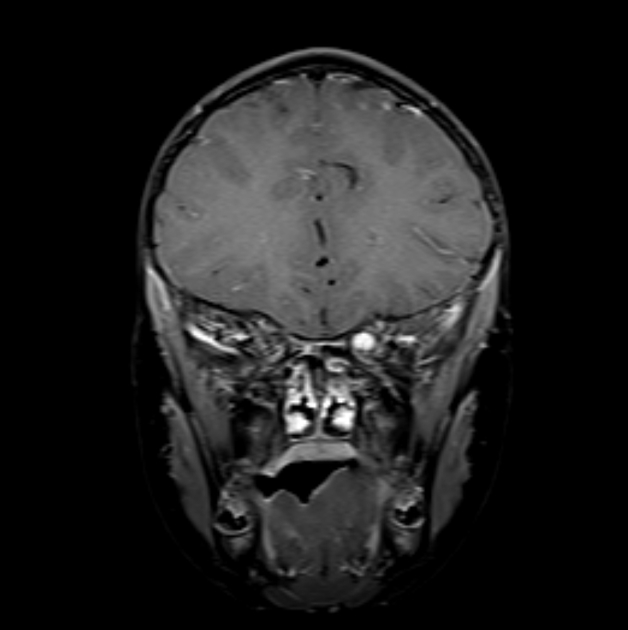
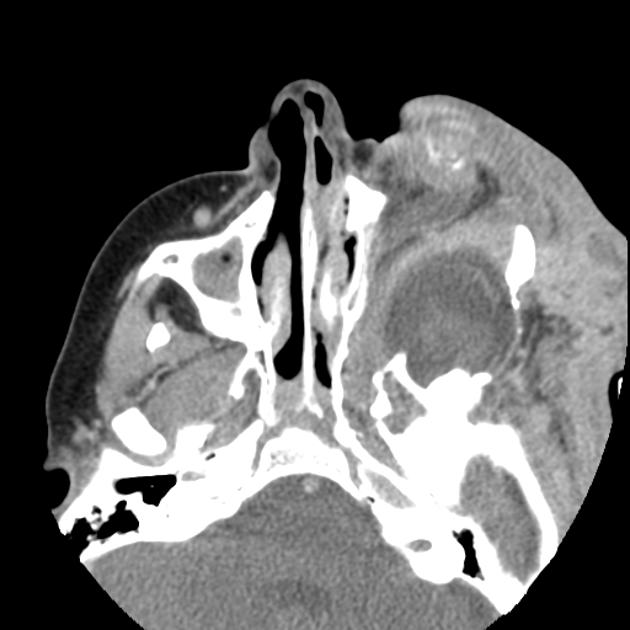
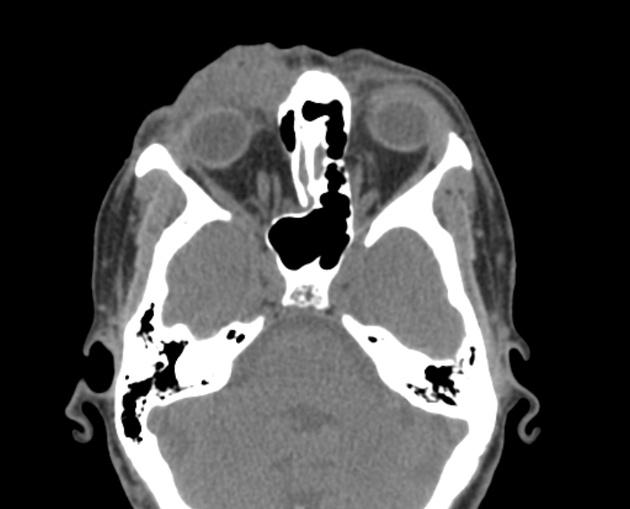
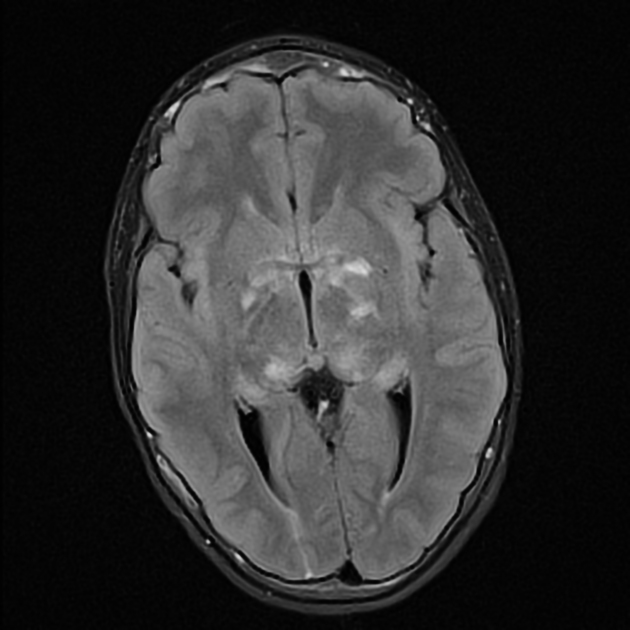
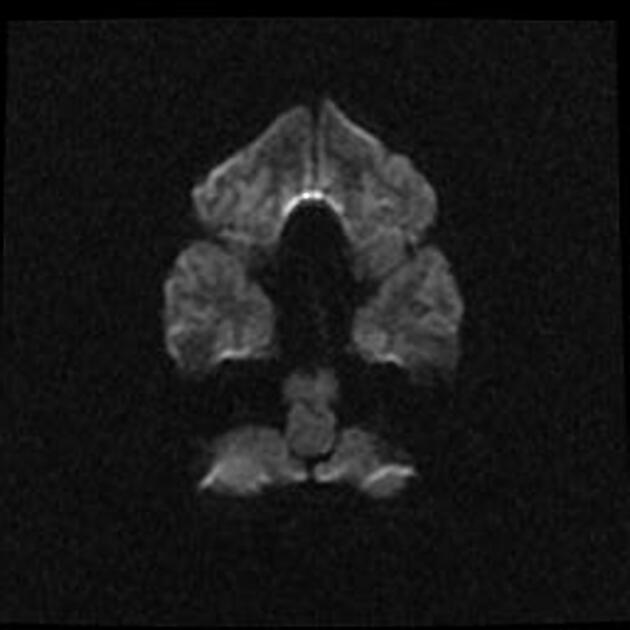
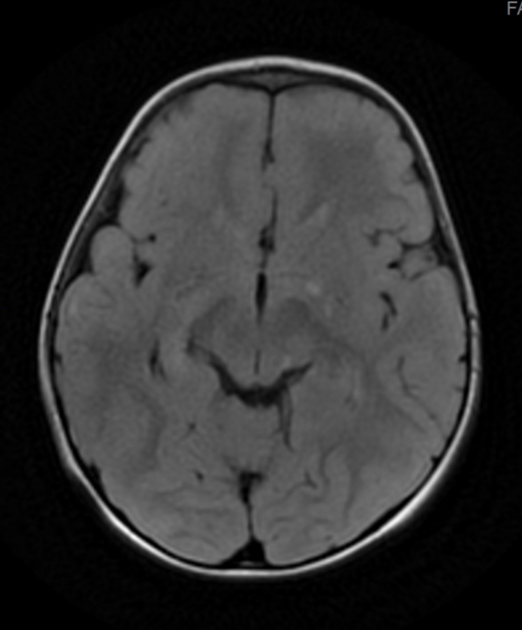
Central nervous system
Manifestations include:
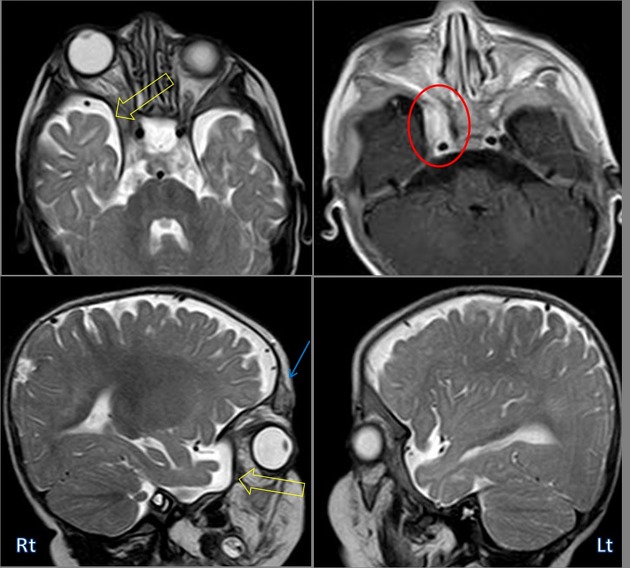
FASI (focal areas of signal intensity): occur in deep white matter and basal ganglia or corpus callosum 5, areas of T2/FLAIR hyperintensity with no contrast enhancement
optic nerve glioma or optic pathway glioma (may manifest as enlarged optic foramen)
progressive sphenoid wing dysplasia
lambdoid suture defects
dural calcification at the vertex
moyamoya phenomenon (rare)
See central nervous system manifestations of NF1 for details.
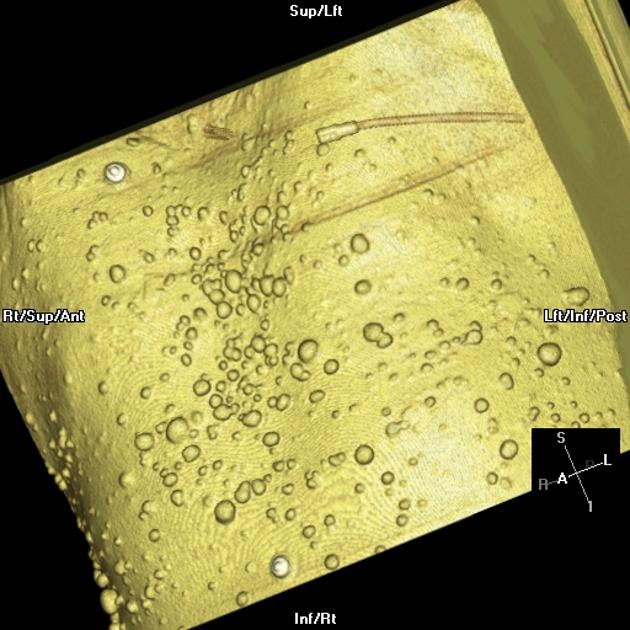
Cutaneous
Manifestations include:
cutaneous and subcutaneous neurofibromas: benign peripheral nerve sheath tumors
See cutaneous manifestations of NF1 for details.
Skeletal
Manifestations include:
posterior vertebral scalloping
hypoplastic posterior elements
ribbon rib deformity, rib notching, and dysplasia
tibial pseudoarthrosis or, less commonly, ulnar pseudoarthrosis
bony dysplasias: especially affecting the tibia
severe bowing, gracile bones 11
multiple non-ossifying fibromas
See musculoskeletal manifestations of NF1 for details.
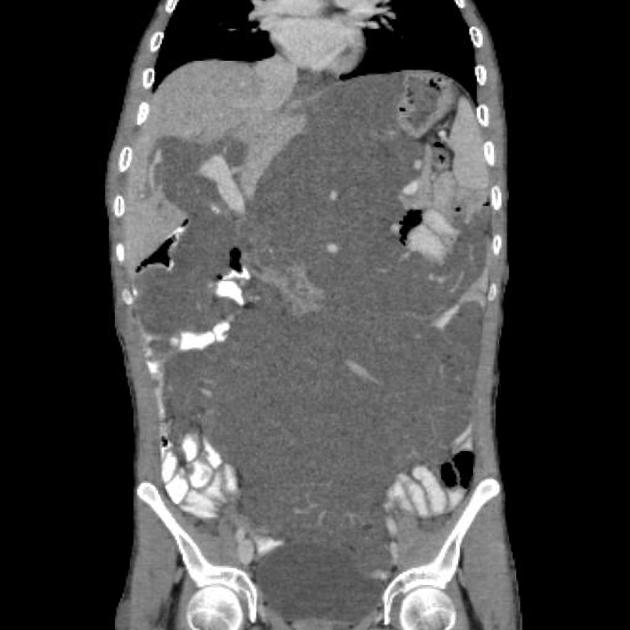
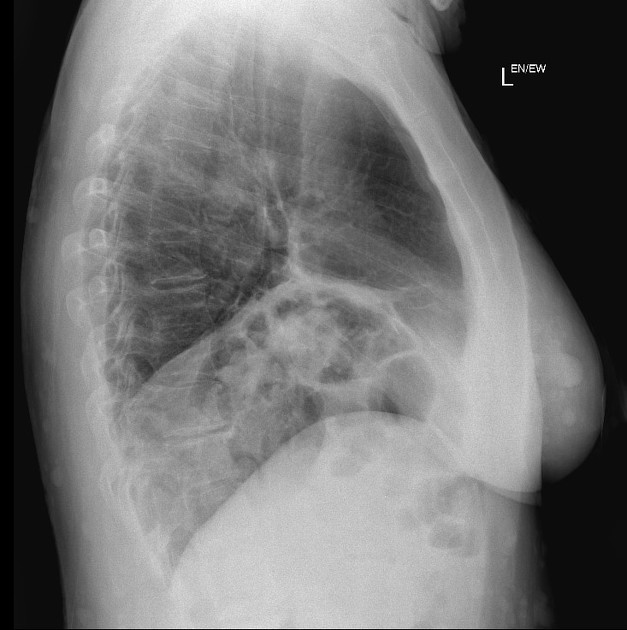
Thoracic
Manifestations include:
-
mediastinal masses
lateral thoracic meningocele: typically on the convex side of scoliosis (through widened neural foramina)
extra-adrenal pheochromocytoma (paraganglioma)
-
lung parenchymal disease: ~20%
diffuse interstitial fibrosis: lower zone
bullae formation: upper zone
secondary pulmonary arterial hypertension and cor pulmonale
See pulmonary manifestations of NF1 for details.
Vascular
Manifestations include:
Treatment and prognosis
No single treatment exists, and a combination of supportive and surgical therapies are employed depending on the specific tumors and anomalies present.
Although prognosis is very variable, overall life expectancy is approximately half that of non-affected individuals. Tumors or cardiovascular complications are the most common causes of mortality 8.
History and etymology
The first name of this condition was von Recklinghausen disease because in 1882, Friedrich von Recklinghausen described cases of neurofibromatosis and recognized it as a nosological entity 14.















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.