
Osteonecrosis of the humeral head, also known as Haas disease, is considered the second most common location for osteonecrosis (following the hip).
On this page:
Clinical presentation
Insidious onset of pain poorly localized and usually severe night and rest. The range of motion is initially preserved. In the later stages a "click" can accompany some movements from joint incongruity, cartilage flap, or a large loose body.
Pathology
It generally develops in the subchondral region. In some patients, osteonecrosis can lead to the collapse of the necrotic subchondral bone, the development of an irregular joint surface, and subsequent joint degeneration.
There are many causes of humeral head osteonecrosis; the most frequent are:
trauma: fracture, fracture-dislocations
metabolic: Gaucher disease
rheumatologic disorders: systemic lupus erythematosus
extrinsic factors: dysbaric conditions (Caisson disease)
alcohol consumption
iatrogenic
-
corticosteroids
recognized as a dominant causative association
corticosteroids cause fat accumulation in the marrow, leading to increased intraosseous hypertension and decreased blood flow
organ transplantation
Classification
Osteonecrosis of the humeral head is staged using the Cruess classification 6.
Radiographic features
Plain radiograph
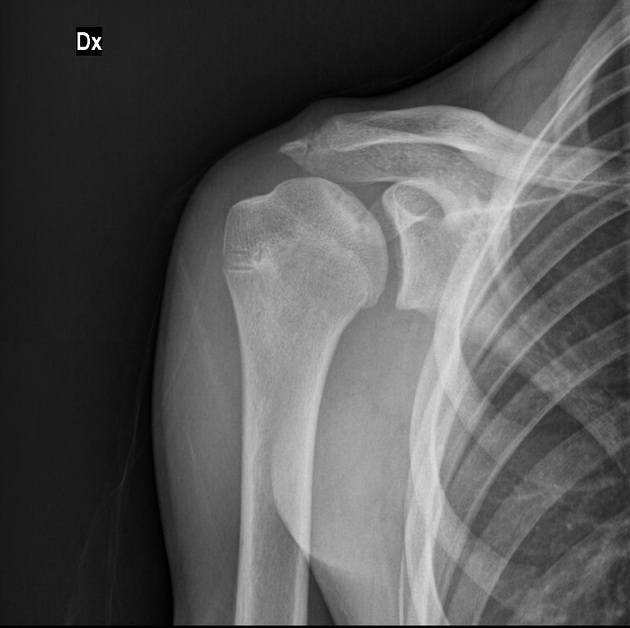
AP, Grashey, axillary and Y projections are typically performed.
Radiographs will be normal in early disease. The most common initial site is the upper middle portion of the humeral head. Early shoulder osteonecrosis shows cystic and/or sclerotic changes in the humeral head. Dense sclerosis on the humeral (or femoral) head in osteonecrosis is called the snowcap sign in radiographs 8.
The presence of a crescent sign is the classic diagnostic feature that in the correct clinical context demonstrates subchondral collapse. This may progress to depression of the articular surface with subsequent arthritic changes.
MRI
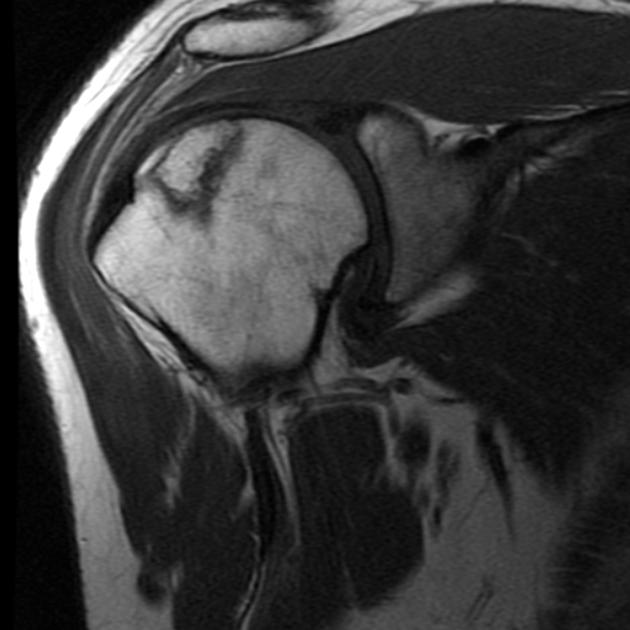
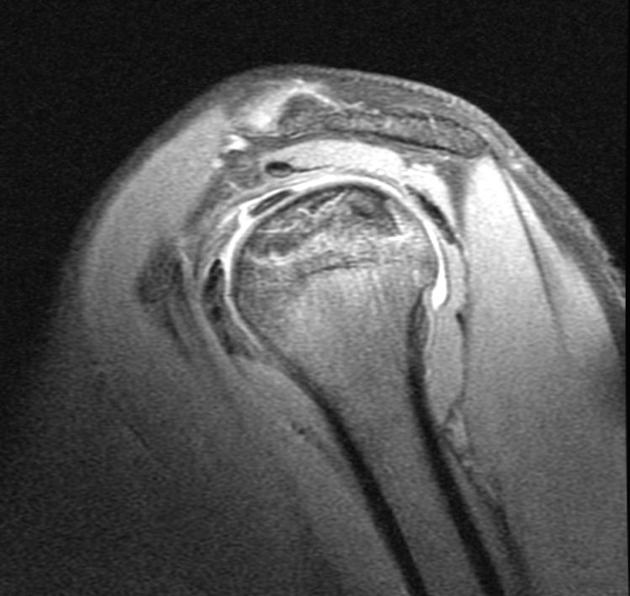
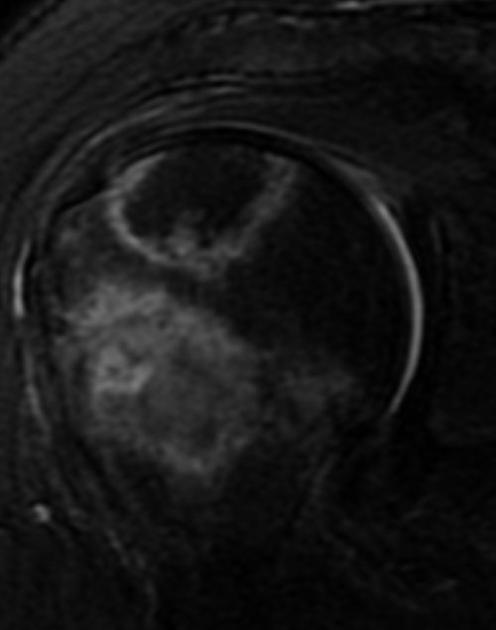
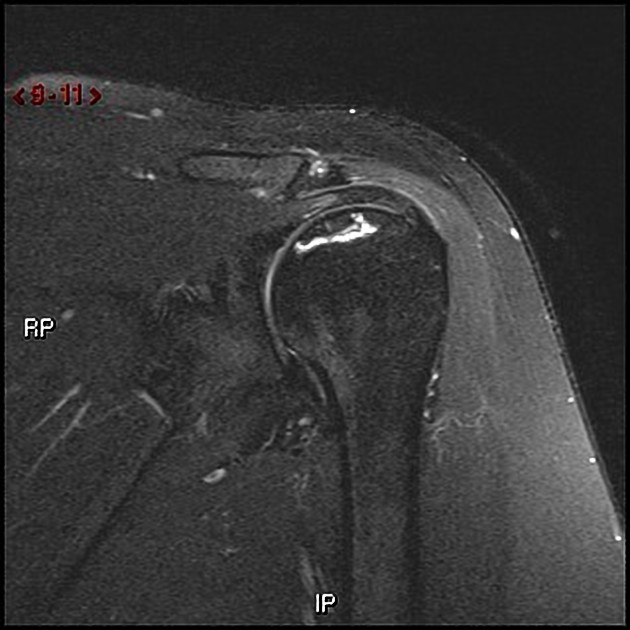
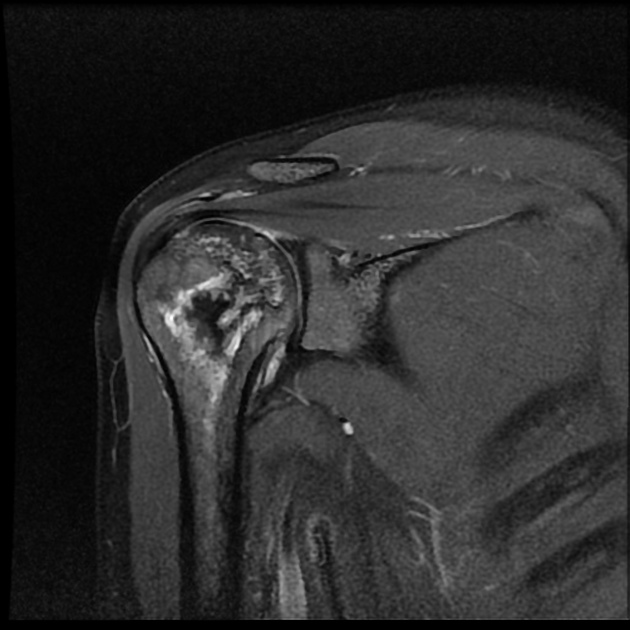
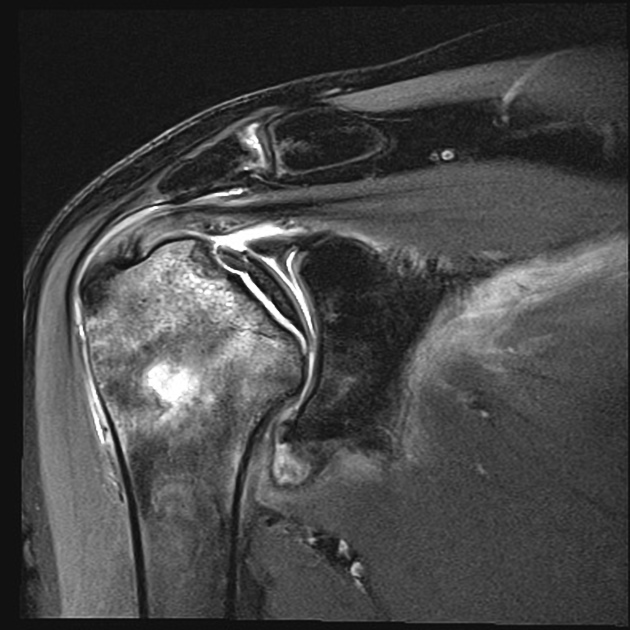
MRI is the preferred imaging modality. The diagnosis of osteonecrosis on MRI is based on band-like abnormal signals:
T1: low signal serpiginous line demarcating the osteonecrosis
T2: double line sign (inner bright line from granulation tissue and outer dark line from sclerotic bone)
Treatment and prognosis
Conservative treatment such as pain medication and physical therapy can be performed for milder cases. Operative procedures include core decompression, shoulder hemiarthroplasty or total shoulder arthroplasty for more severe cases, in particular:
Core decompression of osteonecrosis of humeral head for Stage I and Stage II
Shoulder resurfacing arthroplasty for Stage III
Hemiarthroplasty for Stage III and Stage IV
Total shoulder arthroplasty for Stage V
History and etymology
Dysbaric shoulder osteonecrosis was reported as early as 1911 by Bornstein and Plate. In 1960, Heimann and Freiberger publish the first descriptions of osteonecrosis of the shoulder.







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.