
Pelvic radiographs are a mainstay radiographic examination in trauma imaging. The standard radiographic exam is an AP pelvis, however more specialized projections can be requested to answer specific clinical questions. For a list of the specialized views see the pelvis series article.
On this page:
Systematic review
Choosing a search strategy and utilizing it consistently is a helpful method to overcome common errors seen in diagnostic radiology. The order in which you interpret the radiograph is a personal preference. A recommended systematic checklist for reviewing musculoskeletal exams is soft tissue areas, cortical margins, trabecular patterns, bony alignment, joint congruency, and review areas. Review the entire radiograph, regardless of perceived difficulty. Upon identifying an abnormality, do not cease the review, put it aside and ensure to complete the checklist.
The pelvis radiograph is comprised of the innominate hip bones or os coxae (ischium, pubis and ilium), the sacrum and the proximal femur. Much of the interpretation is down to regions, rings and lines alongside an understanding of traumatic fracture patterns of the pelvic ring.
Soft tissue
Assess all soft tissue structures for any associated or incidental soft tissue signs.
Bony anatomy
The pelvis forms a ring structure, and depending on the mechanism of injury there may be more than one fracture. Bony anatomy assessment frequently involves well known anatomical lines and boundaries for breaks in the cortex.
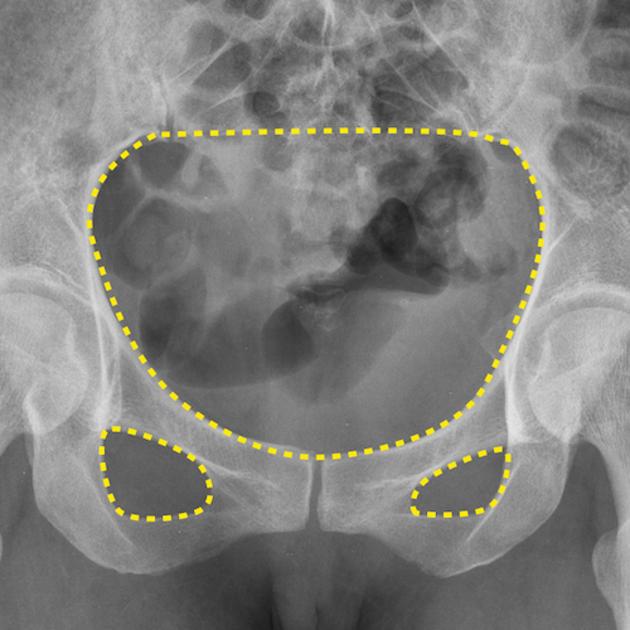
Pelvic rings
carefully trace the inner cortex of the pelvic ring
trace in the inner cortext of the two obturator foramina
if one of the rings are disrupted, look for a second fracture
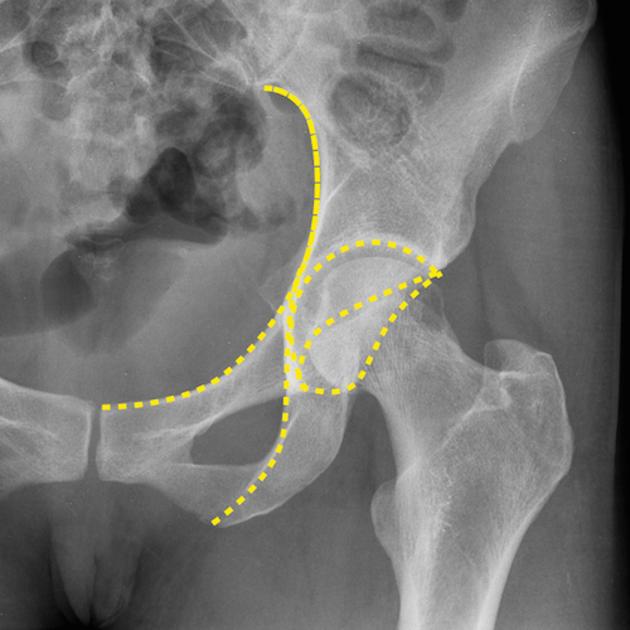
Acetabulum
The acetabulum is a complex three dimensional innominate bone that comprises an anterior and posterior column and a roof. Thorough assessment of the acetabulum (in the absence of CT) should include oblique internal and external pelvis views (Judet views). The following lines, known as Letournel lines, are useful:
-
disruption suggests a fracture involving the anterior column
-
disruption suggests a fracture involving the posterior column
acetabular roof
anterior rim
posterior rim
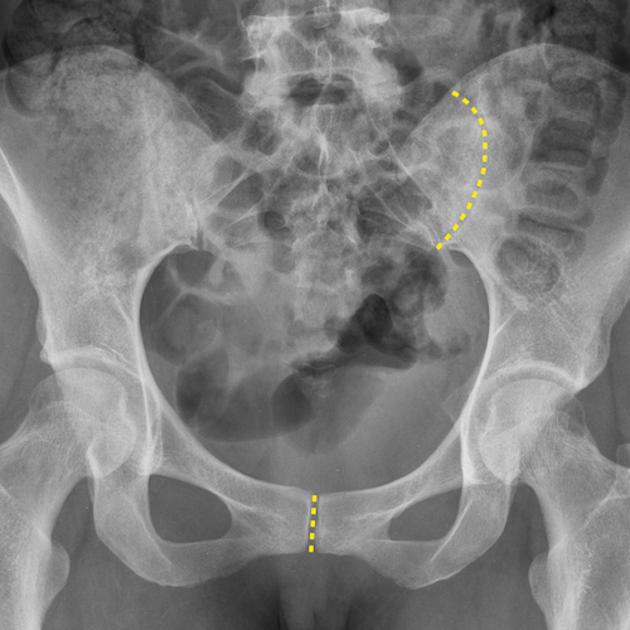
Sacral foramina
trace the arcuate lines of the sacrum, they should be smooth and very symmetrical
sacral fractures are seldom isolated
Proximal femur
-
the cortex of femoral head, neck, greater, and lesser trochanter should be smooth with normal trabecular pattern on AP and lateral
if cortical disruption, trabecular pattern disruption or transverse sclerosis, think fractured proximal femur
-
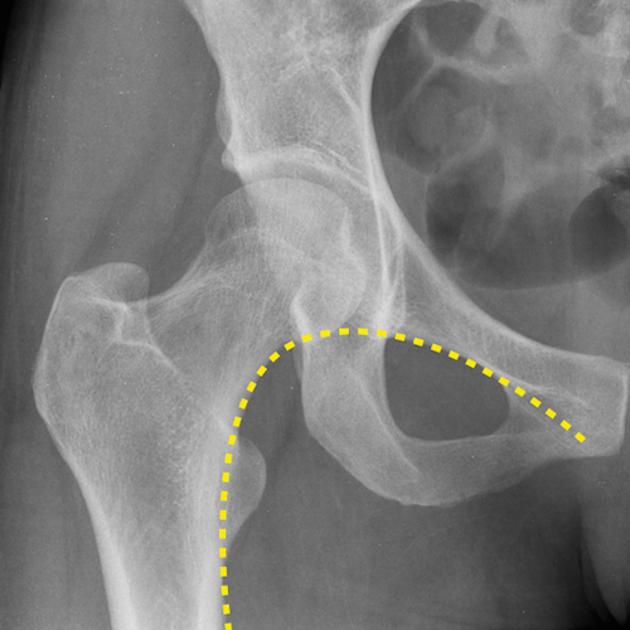
trace the Shenton line
if line disruption, think fractured proximal femur
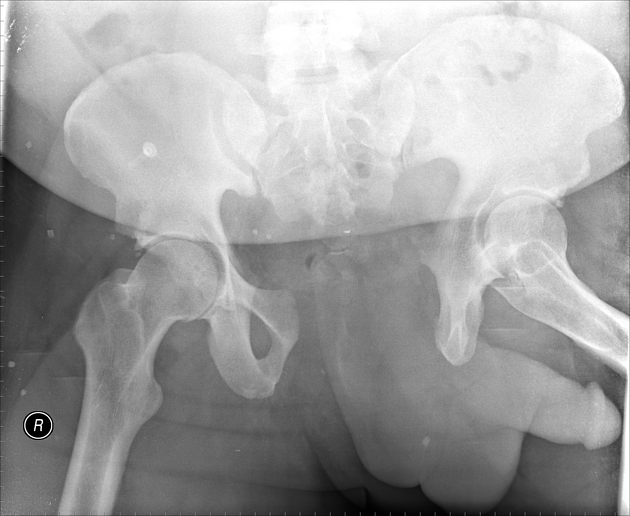
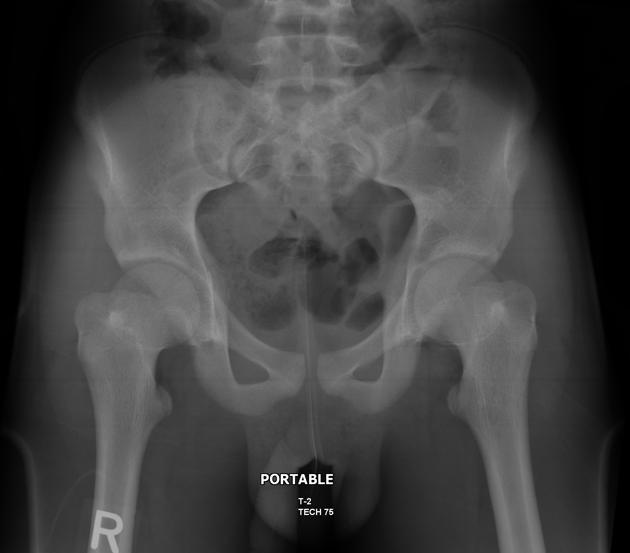
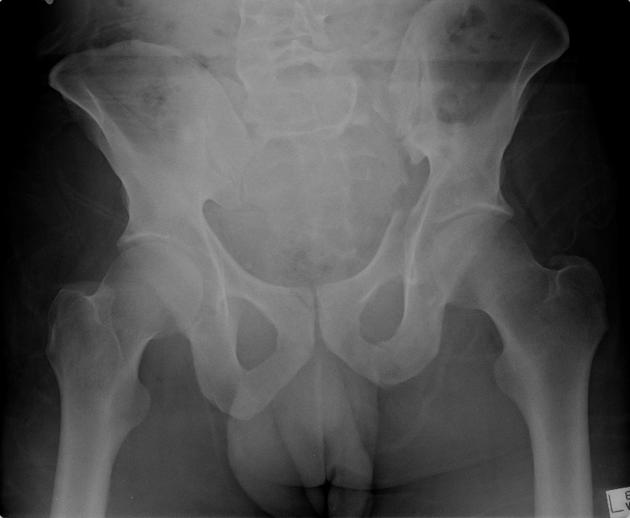
Pediatric pelvis
The pediatric pelvis has added complexity based on patient age, the aforementioned checks still hold true however one must also consider:
-
line drawn along the superior edge of the femoral neck, which is useful in detecting early slipped upper femoral epiphysis
Alignment
Joint spaces
the sacroiliac joints should be symmetrical, joint space range 2-4 mm
the symphysis pubis joint space should be ≤5 mm
if either joint space is widened, think main pelvic ring fracture
Pediatric pelvis
Consider the alignment of the femoral head using the following:
Common pathology
Proximal femoral fracture
typically elderly osteoporotic females
fall in elderly or high-energy blunt trauma
Intracapsular
-
fracture site within the joint capsule
subcapital (most common), transcervical, or basicervical
-
high risk of disruption of the blood supply to the femoral head
displaced intracapsular fractures are associated with delayed union, non-union, or avascular necrosis
Extracapsular
-
fracture line distal to the attachment of the femoroacetabular joint capsule
intertrochanteric (most common) or subtrochanteric
Pubic ramus fracture
40% of all pelvic fractures
isolated fracture of superior or inferior ramus most common stable pelvic injury
-
mechanisms:
fall in elderly
exercise-induced stress fractures
more: pubic ramus fracture
Complex pelvic ring fracture
fracture at one site often associated with a second
a double break represents an unstable injury
high energy blunt trauma
requires CT evaluation
Acetabular fracture
bimodal distribution: young (high energy) and elderly (poor bone quality)
impaction of femoral head, lateral compression or axial loading
75% associated with femoral head subluxation/dislocation; frequently comminuted
more: acetabular fracture
Head of femur dislocation
uncommon
80% posterior
high energy blunt trauma
associated with posterior rim acetabular fractures
Don’t miss…
Apophyseal avulsion
typically adolescent athletes
repeated or sudden muscle contraction
ischial tuberosity avulsion (hamstring insertion) most common
Sacral fracture
common in pelvic ring fractures
-
mechanisms:
fall in elderly
high-energy blunt trauma
frequently missed
25% associated with neurologic injury
more: sacral fracture












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.