
Rhabdomyosarcomas of the head and neck represent a large proportion (~40%) of all rhabdomyosarcomas and are the most common soft tissue sarcomas of the head and neck. For a general discussion of this tumor, please refer to rhabdomyosarcoma.
On this page:
Pathology
They are usually of the embryonal cell subtype, essentially only seen in children, and are classified by location:
orbital rhabdomyosarcoma: good prognosis (90% long-term survival)
para-meningeal rhabdomyosarcoma: worse prognosis (50% long term survival)
other head and neck locations
Middle ear rhabdomyosarcomas are rare, accounting for only 7% of head and neck rhabdomyosarcomas. They typically present similarly to chronic otomastoiditis and are usually diagnosed too late for curative treatment. Cranial nerve involvement is present in 30% at the time of diagnosis.
Microscopic appearance
Histologically, rhabdomyosarcomas are low-grade small round blue cell tumors. Ewing sarcoma, neuroblastoma, and lymphoma share similar characteristics that make histopathologic differentiation of rhabdomyosarcoma hard.
Radiographic features
Ultrasound
Rhabdomyosarcomas resemble neuroblastomas in echotexture and often demonstrate low to medium echogenicity. With color Doppler, there is variable internal vascularity.
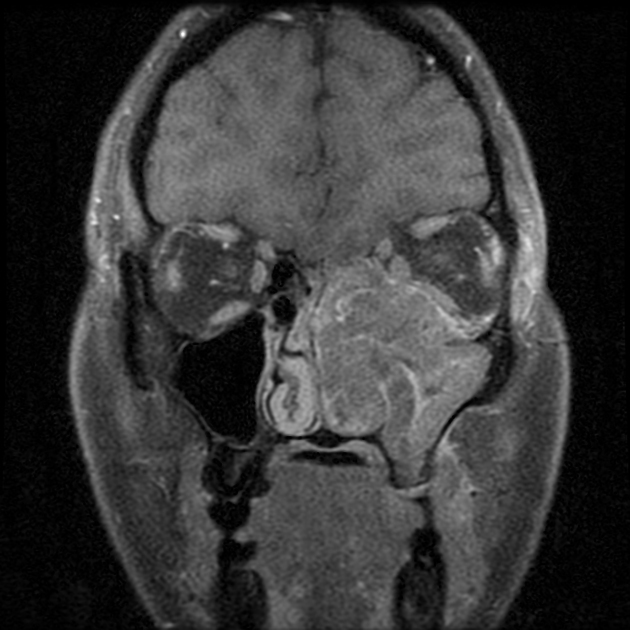
MRI
T1: isointense to slightly hyperintense
T2: hyperintense
T1 C+: marked contrast enhancement
+/- intralesional hemorrhage or necrosis
+/- diffusion restriction
Radiology report
As the differential diagnosis is vast, and the imaging findings are non-specific, it is useful to describe in detail the:
location
involvement of adjacent compartments
perineural, vascular, and osseous involvement
presence of lymphadenopathy
Treatment and prognosis
Treatment depends on the location and disease extent, with orbital and non-parameningeal head and neck locations having a better prognosis. Chemotherapy is first line for the treatment of rhabdomyosarcomas, with radiation therapy and surgery utilized for local tumor control.
Differential diagnosis
The differential diagnosis for more superficial non-parameningeal locations includes:
fibrosarcoma
The differential diagnosis for deeper parameningeal locations includes:
hemangioendothelioma
The sonographic differential also includes:
fibrosarcoma



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.