
Lymphadenopathy is quite common, and it can be challenging to differentiate malignant lymphadenopathy from reactive nodal enlargement.
Several gray scale and color Doppler features favor malignancy in a lymph node 1,7-9.
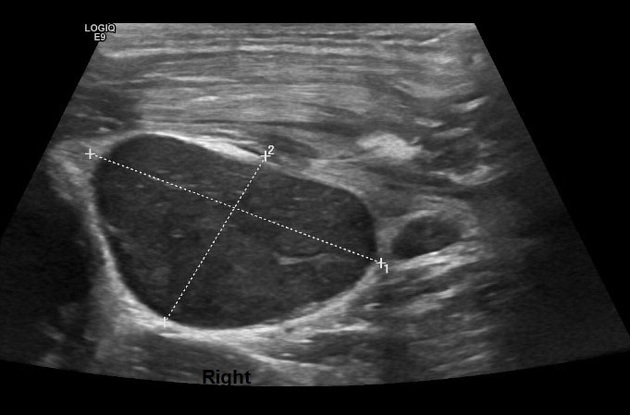
Gray scale parameters that favor malignancy
size: larger - more likely malignant
shape: round, long axis:short axis <2
echogenicity: predominantly hypoechoic although metastatic lymph nodes from papillary thyroid carcinoma tend to be hyperechoic due to the intranodal deposition of thyroglobulin
heterogeneous echotexture
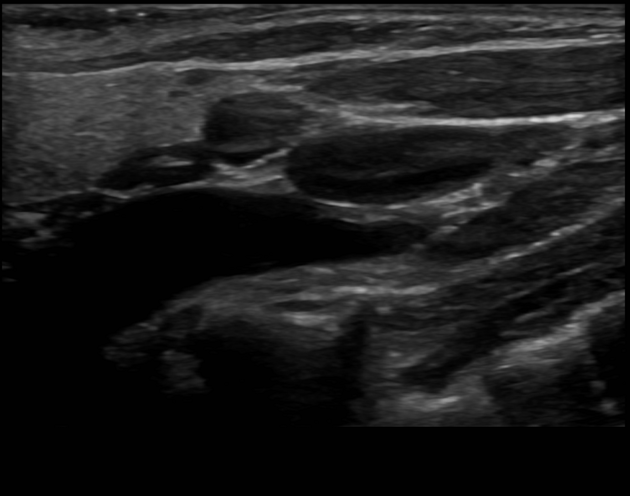
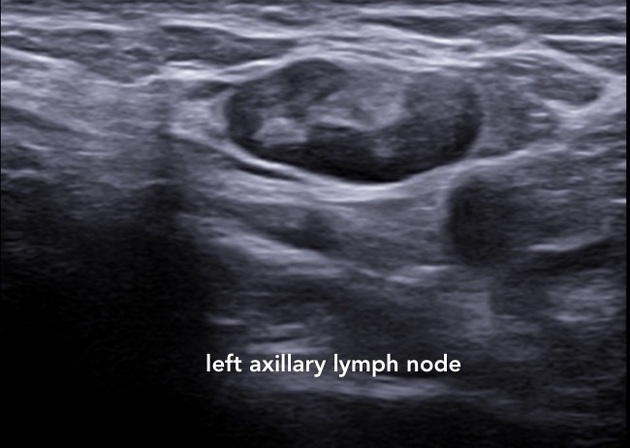
loss of central fatty hilum/thinning of hilum
eccentric versus concentric thickening of cortex
presence of microcalcifications
necrosis: cystic/coagulative
ill-defined capsular margins: invasion
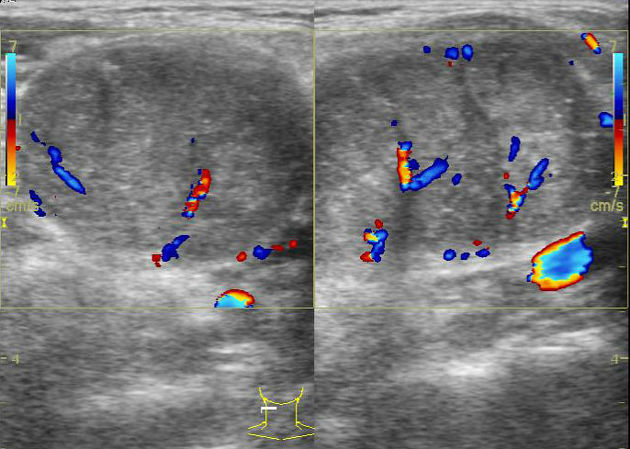
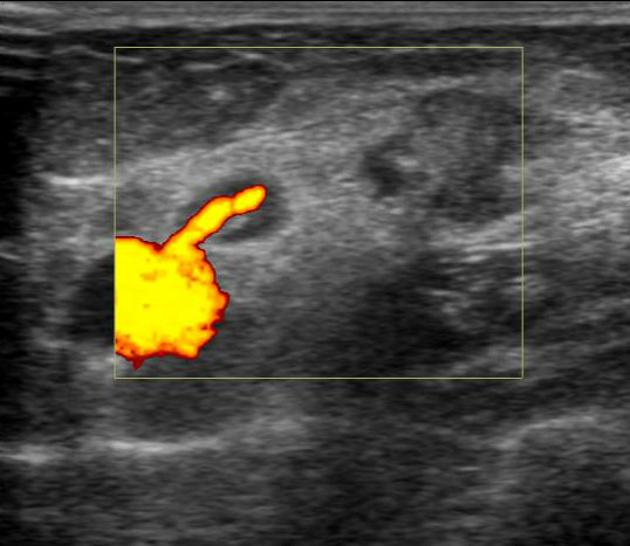
Color/power Doppler features that favor malignancy
peripheral/mixed peripheral: central blood vessels
high resistance waveform
RI >0.8, PI >1.5
aberrant vessels: displaced parent vessels, subcapsular vasculature, non-perfused areas, non-tapering vessels
The increase in resistivity in a malignant lymph node is attributed to increased cellularity within an infiltrated lymph node. However, malignant lymph nodes with necrotic change may show low resistance flow due to loss in the cellularity following necrosis and this needs to be kept in mind while interpreting this sign.
When used in combination the above signs can help differentiate a malignant lymphadenopathy from reactive nodal enlargement.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.