
Achondroplasia is a congenital genetic disorder resulting in rhizomelic dwarfism and is the most common skeletal dysplasia. It has numerous distinctive radiographic features.
On this page:
Epidemiology
It occurs due to sporadic mutations in the majority of cases but can be inherited as an autosomal dominant condition. Homozygous achondroplasia is lethal.
There is a prevalence of approximately 1 in 25,000-50,000 births with males affected more frequently than females 18.
Clinical presentation
Achondroplasia is the most common cause of short-limb dwarfism. Patients are of normal intelligence and motor function, presenting with delayed motor milestones. They may have specific neurologic deficits. Stenosis of the foramen magnum can, for example, present with difficulty swallowing or snoring.
Pathology
The disease results from a mutation in the fibroblast growth factor gene 3 (FGFR3) located on chromosome 4p16.3 which causes abnormal cartilage formation. These are cell surface receptors comprised of an extracellular domain with three immunoglobulin-like regions, a transmembrane domain and an intracellular tyrosine kinase 19.
The mutation to the FGFR3 gene in achondroplasia is a gain of function mutation with constitutive activation of an inhibitory signal 19,20. All bones that form by endochondral ossification are affected. Bones that form by membranous ossification are not affected, thus allowing the skull vault to develop normally.
Associations
SADDAN syndrome: severe achondroplasia with developmental delay and acanthosis nigricans
Radiographic features
Almost all the bones of the skeleton are affected, and hence all parts of the body have bony changes with secondary soft tissue changes. Antenatally it is difficult to diagnose achondroplastic features until the 3rd trimester 13.
Ultrasound
Antenatally detectable sonographic features include:
-
short femur length measurement: often well below the 5th centile
the femur length (FL) to biparietal diameter (BPD) is taken as a useful measurement
trident hand 11: 2nd, 3rd, and 4th fingers appear separated and similar in length
separation of 1st, 2nd, 3rd, and 4th fingers
protruding forehead: frontal bossing
depressed nasal bridge
Plain radiograph / CT / MRI
Features on radiographs, CT, and MRI are similar and discussed together here.
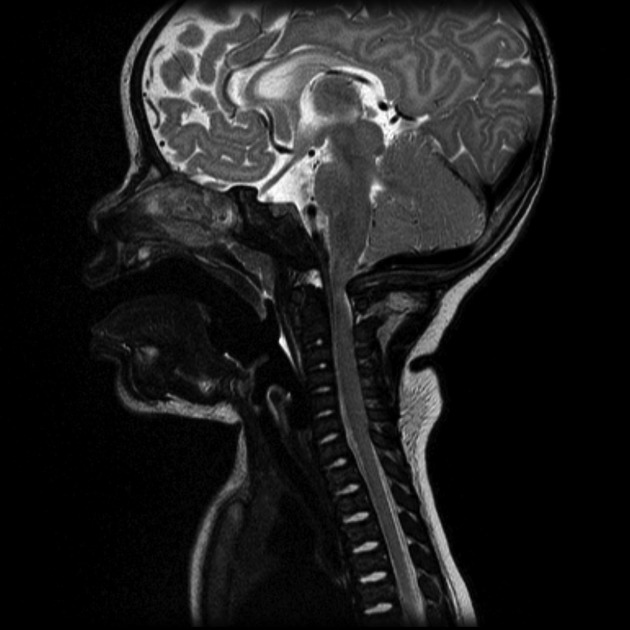
Cranial
relatively large cranial vault with small skull base
frontal bossing with the depressed nasal bridge (midfacial retrusion) 19
narrowed foramen magnum
relative elevation of the brainstem resulting in a large suprasellar cistern and vertically-oriented straight sinus
communicating hydrocephalus (due to venous obstruction at sigmoid sinus)
large anterior fontanelle in infancy; may persist to 5 or 6 years of age 19
Also, see the achondroplastic base of skull abnormalities for further discussion.
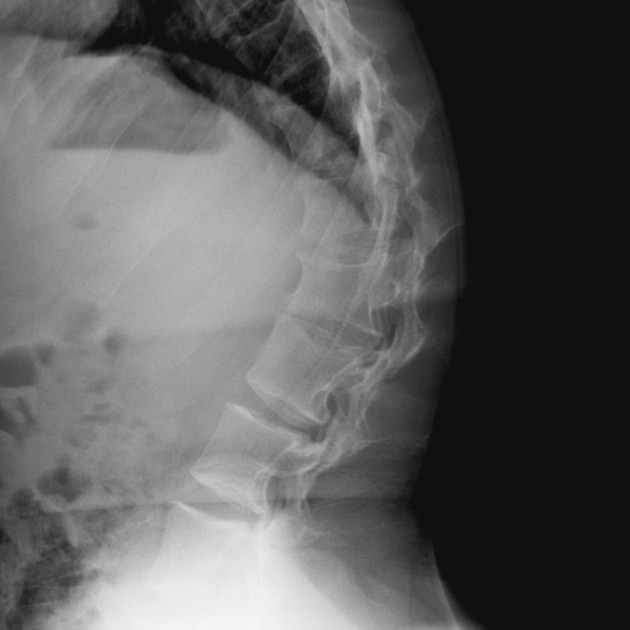
Spinal
progressive decrease in the interpedicular distance in the lumbar spine: decreased L5-S1 is pathognomonic
gibbus: thoracolumbar kyphosis with bullet-shaped/hypoplastic vertebra (not to be confused with Hurler syndrome)
short pedicle canal stenosis
widening of intervertebral discs 8
an increased angle between the sacrum and lumbar spine
Chest
anterior flaring of the ribs
anteroposterior narrowing of the ribs
Pelvis and hips
horizontal acetabular roof (decreased acetabular angle)
small squared (tombstone or mickey mouse ear) iliac wings
small trident acetabulum
short sacroiliac notches
Limbs
metaphyseal flaring 8: can give a trumpet bone type appearance
the femora and humeri are particularly shortened (rhizomelic shortening)
long fibula: the fibular head is at the level of the tibial plateau
bowing to mesial segment of legs 19
the limbs may also appear thickened but are in fact normal in absolute terms; thickening is perceived due to reduced length
chevron sign 16,17
the metacarpal and metatarsal bones, and in some cases the proximal phalanges, are short and of similar length
pseudoepiphyses or accessory epiphyses22
A useful mnemonic can be found here.
Treatment and prognosis
There is often a danger of cervical cord compression due to narrowing of the foramen magnum.
Treatment varies and is usually orthopedic, particularly to correct kyphoscolioses, as well as neurosurgical, to decompress the foramen magnum or shunt hydrocephalus 6,7.
Overall prognosis is good, with near-normal life expectancy in heterozygous individuals. When homozygous, the condition is fatal due to respiratory failure 7.
History and etymology
Achondroplasia literally means "without cartilage formation", although the pathology is impaired endochondral ossification (see Pathology section above).
Differential diagnosis
The differential diagnosis is that of other less common skeletal dysplasias, including 6:
chondroectodermal dysplasia (Ellis-van Creveld syndrome)
See also
causes of limb bowing: general differential for (lower) limb bowing
rhizomelic dwarfism: general differential for rhizomelic limb shortening












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.