
Boerhaave syndrome refers to an esophageal rupture secondary to forceful vomiting and retching.
On this page:
Epidemiology
It tends to be more prevalent in males, with alcohol use a risk factor. The estimated incidence is ~ 1:6000.
Clinical presentation
Boerhaave syndrome is often associated with the clinical triad (Mackler triad) of vomiting, chest pain and subcutaneous emphysema. Other symptoms include epigastric pain, back pain, dyspnea and shock. This condition is universally fatal if left untreated 12.
Pathology
It is thought to occur due to a forceful ejection of gastric contents in an unrelaxed esophagus against a closed upper esophageal sphincter/cricopharyngeus. The tears are vertically oriented, 1-4 cm in length. Approximately 90% occur along the left posterolateral wall of the distal esophagus, 3-6 cm above the esophageal hiatus of the diaphragm 10.
Radiographic features
Plain radiograph
Chest radiograph findings are often non-specific, and the radiograph may be normal. The classic chest radiographic findings include pneumomediastinum, left pleural effusion and left pneumothorax. Gas may also be seen within the soft tissue spaces of the chest wall and the neck.
Another sign that may be present is the Naclerio V sign, which describes a focal, sharply marginated region of paraspinal radiolucency on the left side immediately above the diaphragm 3.
Fluoroscopy
On contrast swallow:
up to 10% of patients have a false negative result 3,10
may directly demonstrate contrast medium leakage, often at a supradiaphragmatic level
submucosal contrast collections
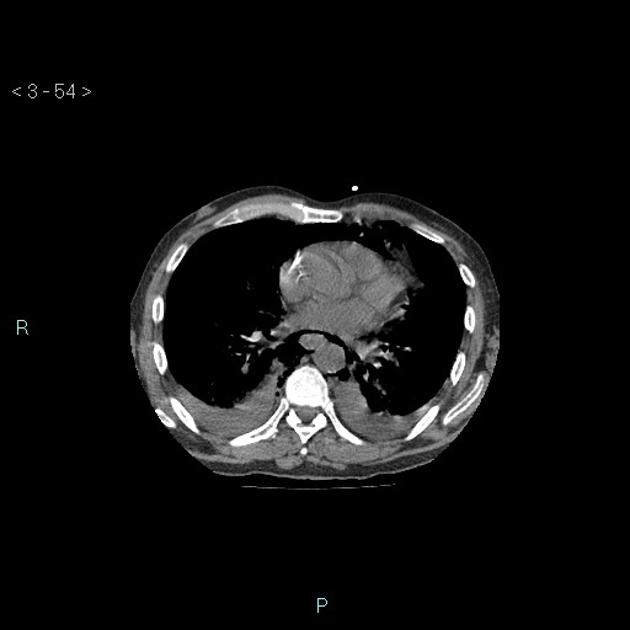
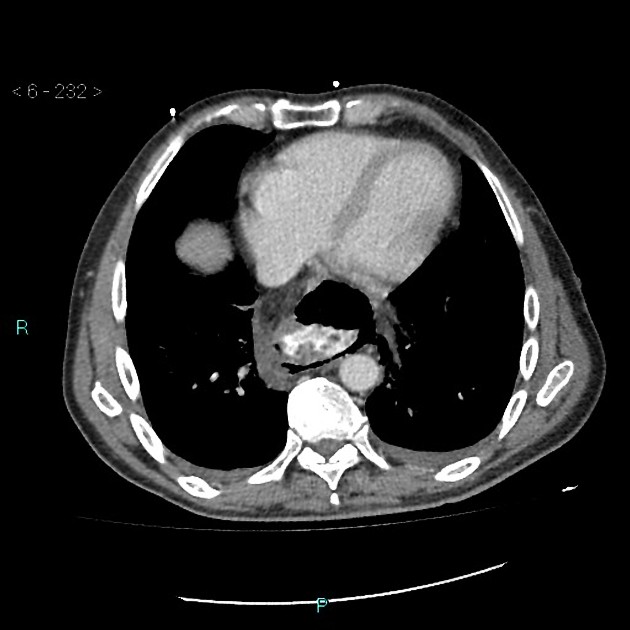
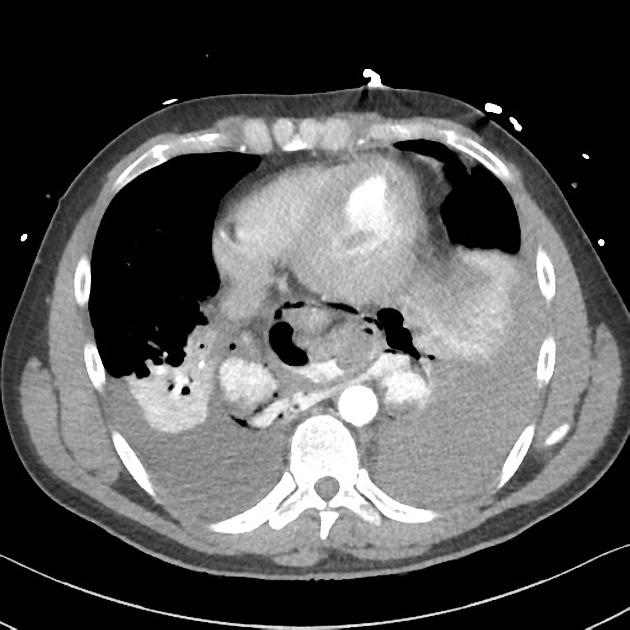
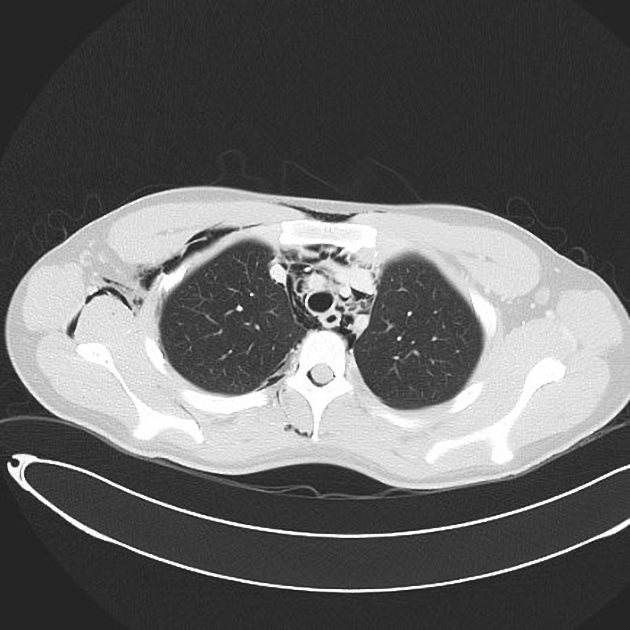
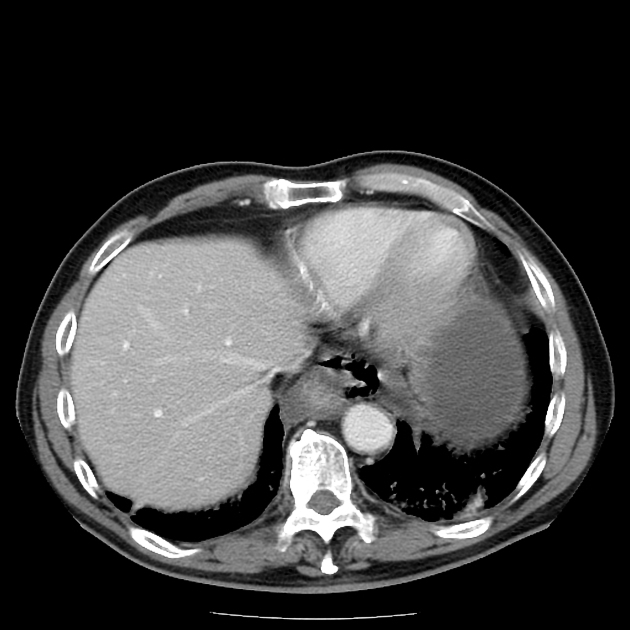
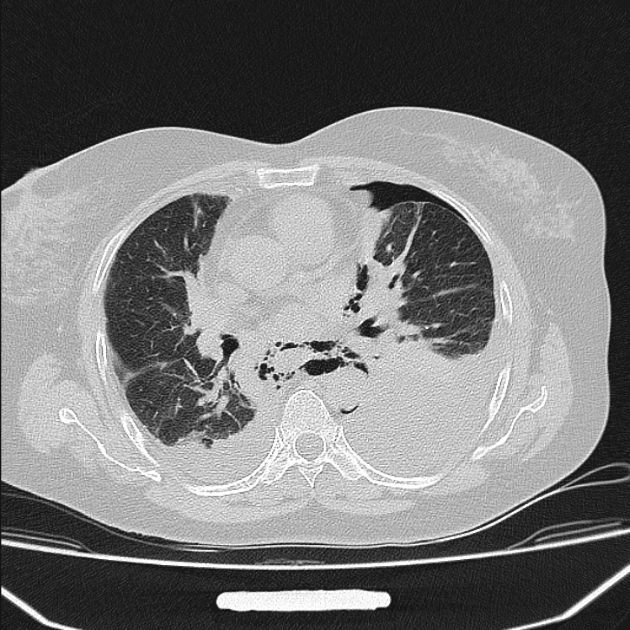
CT
Features reported on unenhanced CTs include the presence intramural hematoma with a typical localization and peri-esophageal air collections indicating esophageal perforation 2. Post contrast CT may show direct contrast leakage/tracks and esophageal wall thickening.
Other reported findings include:
periaortic gas tracks
pneumothorax: has a left sided predilection
pleural effusion: usually left sided
mediastinal fluid collections
oral contrast extravasation from the esophagus
gas within soft tissue spaces of the chest wall and neck, and around the great vessels
gas extending into spinal epidural, peritoneal and retroperitoneal spaces
Differential diagnosis
esophageal perforation from iatrogenic injury
Mallory-Weiss tear: partial thickness tear
epiphrenic diverticulum: mimicking pneumomediastinum
esophageal or pulmonary malignancy causing esophagopleural fistula
Treatment and prognosis
Mediastinal infection and sepsis can be life-threatening (mortality as high as 35% 1), especially if there is a delay in diagnosis. Surgery is the gold standard treatment. However, there is an emerging use of conservative methods, namely esophageal stenting.
Mortality can be as low as 6.2% when identified and treated in the first 24 hours 11. This condition is universally fatal if left untreated 12.
Complications
History and etymology
It is named after Hermann Boerhaave (1668-1738), a Dutch professor of clinical medicine 4,8. The syndrome was described after the case of Dutch Admiral Baron Jan von Wassenaer, who died of the condition.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.