
Brain death (or death by neurological criteria) refers to the irreversible end of all brain activity and is usually assessed clinically. Radiographic testing may be used as additional support for a clinical diagnosis of brain death, such as when clinical tests are impossible to perform, e.g. facial or ocular trauma, precluding brainstem function assessment.
As the diagnosis of brain death is considered equivalent to cardiac death in many jurisdictions 4 and it allows organ donation for transplantation or withdrawal of life support, most countries have specific and varied related legal standards and practice guidelines 2,10.
It should be noted that brain death imaging is not synonymous with identifying extensive global hypoxic-ischemic injury.
Radiographic features
Most imaging tests for brain death rely on the absence of cerebral blood flow as a surrogate for brain death. This can be assessed by a number of modalities including catheter angiography, nuclear medicine examinations, and to a lesser degree CT angiography, MRI angiography and ultrasound.
It is important to note that not all modalities and examinations are approved for the legal determination of brain death and that this will vary from country to country.
Furthermore, it is essential to realize that the absence of brain perfusion implies brain death, but the converse is not true. In situations where intracranial pressure is not sufficiently elevated, perfusion can continue to occur even though there may be profound global brain infarction. This is, for example, encountered in patients who have large skull defects (traumatic or iatrogenic, e.g. craniectomy for decompression) leading to false negatives 12.
Ultrasound
Transcranial Doppler sonography (TCD) has been used as an ancillary modality to provide further clinical support by detecting the presence of cerebral circulatory arrest, although it is not uniformly recognized as a valid alternative. Features include:
reverberant or oscillating flow in the MCA vessels has been reported 8
loss or reversal of diastolic flow in the MCA/ICA
low acceleration time in the MCA
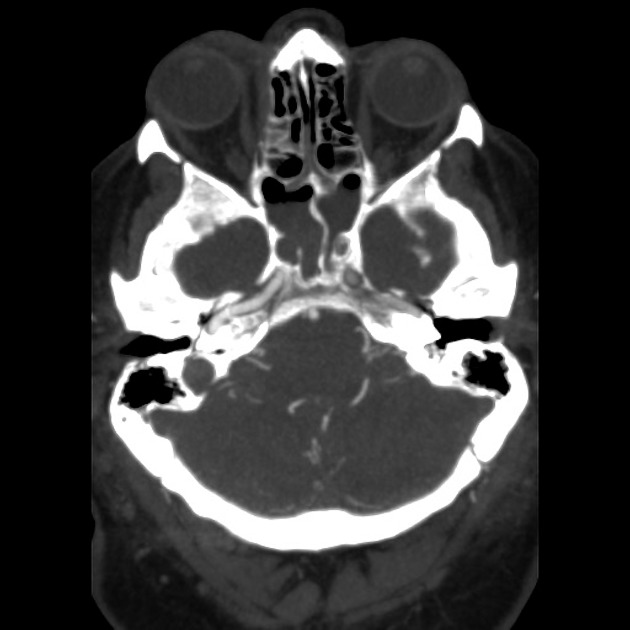
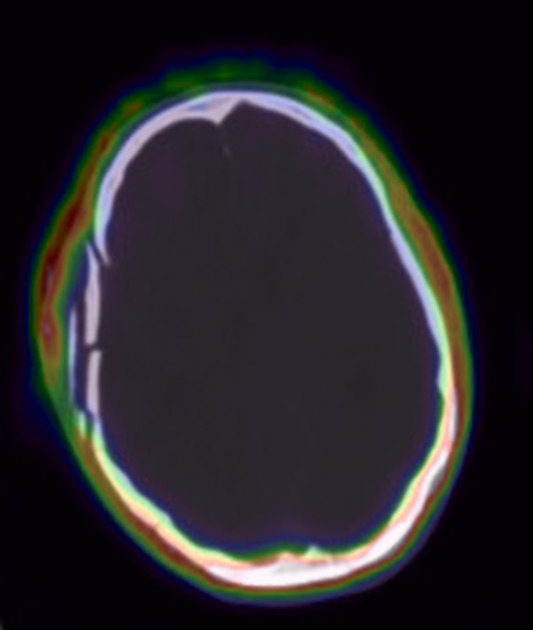
CT
Although CT may demonstrate extensive ischemic damage (e.g. reversal sign, pseudosubarachnoid hemorrhage, cerebral edema, and herniation), as these are more or less subjective, only CT angiography is recognized as a potential alternative to angiography and nuclear medicine studies in some jurisdictions 13-15.
CT angiography relies upon the non-opacification of intracranial vessels, and the vessels that are chosen can affect the sensitivity and specificity of the test 15.
It is also crucial to note that the timing of the study is different to a normal diagnostic study where the aim is to image as early as possible during the arterial phase to avoid excessive venous opacification. When intracranial perfusion is abnormal, such a routine study may result in false positives 15. Thus it is recommended that CT angiography in this setting is delayed to 60 seconds post-injection to allow even the slowest perfusion to be detected 15. In some cases, persistent contrast filling within the proximal cerebral arteries but not in the cortical branches may be demonstrated (stasis filling), which does not reflect true cerebral perfusion 16.
No internationally agreed upon CTA criteria for brain death are available with a variety of point systems and criteria being proposed. Vessels that can be assessed for non-opacification include 3,15:
internal carotid artery above the level of the anterior clinoid processes
vertebral arteries after they have entered the dura, and basilar artery
cortical branches (M4) of the middle cerebral artery 3
UK 2023 Consensus
In 2023 various UK bodies including the Faculty of Intensive Care Medicine, British Society of Neuroradiologists and the RCR published a consensus document on the use of CT angiography as ancillary testing for death by neurological criteria (DNC) 17,18. This is recommended when a comprehensive neurological examination or confounding conditions cannot be performed or excluded. This imaging assessment uses the 4-point criteria described by Frampas 3.
Three phases of imaging are recommended:
unenhanced phase (to identify pre-existing vessel hyperdensity)
20 seconds following contrast administration (to confirm head and neck contrast delivery in the extracranial superficial temporal arteries)
60 seconds following contrast administration (a positive scan result confirming DNC with absolutely no opacification of the bilateral cortical MCA (M4) branches, and no opacification of the internal cerebral veins bilaterally)
This consensus is for adult patients only (not pediatric patients). This is also not supported in cases receiving extracorporeal membrane oxygenation (ECMO).
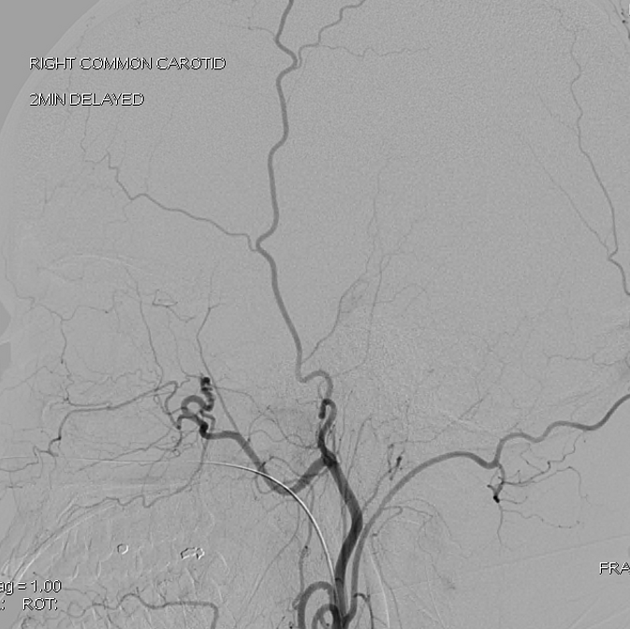
Angiography (DSA)
considered the gold standard imaging test, with near 100% sensitivity and specificity 4,13
shows no forward flow above the terminal internal carotid arteries
contrast should be seen in the external carotid artery branches
flow may be seen up to the supraclinoid internal carotid artery as the ophthalmic artery will continue to flow even if the intracranial pressure is very high
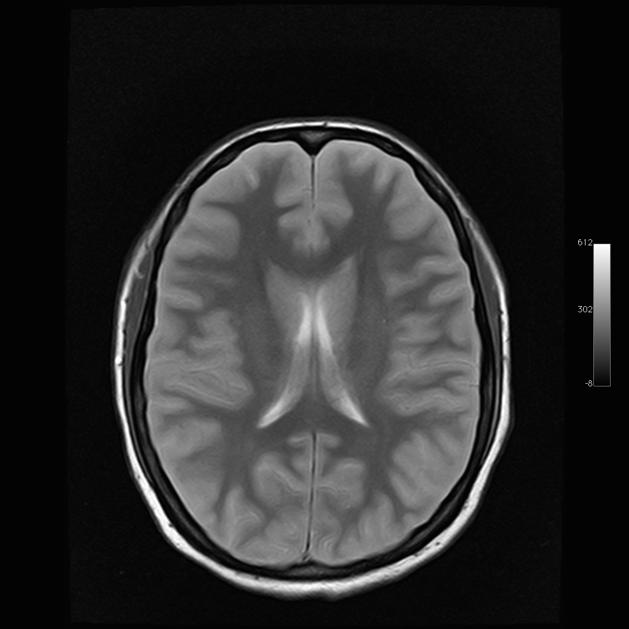
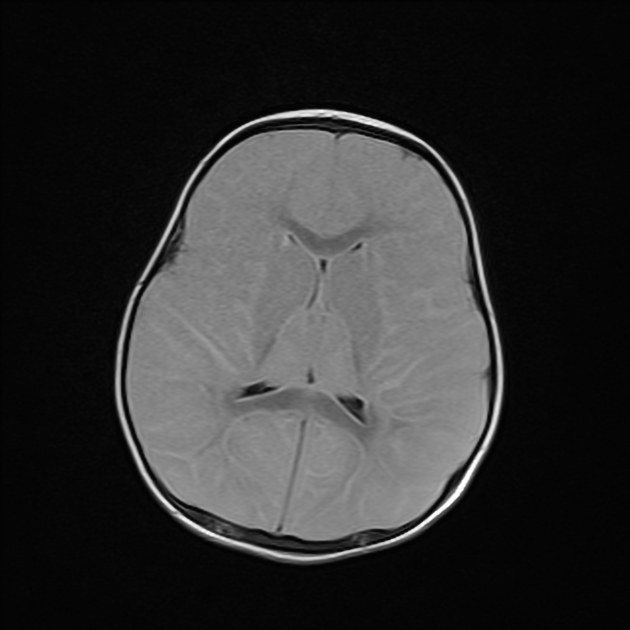
MRI
Although MRI can demonstrate extensive ischemic change more accurately than CT, only MR angiography has been proposed as a potential ancillary test for the diagnosis of brain death, using similar criteria to CT angiography 5,6,13,14. However, MRI is generally not recommended 14.
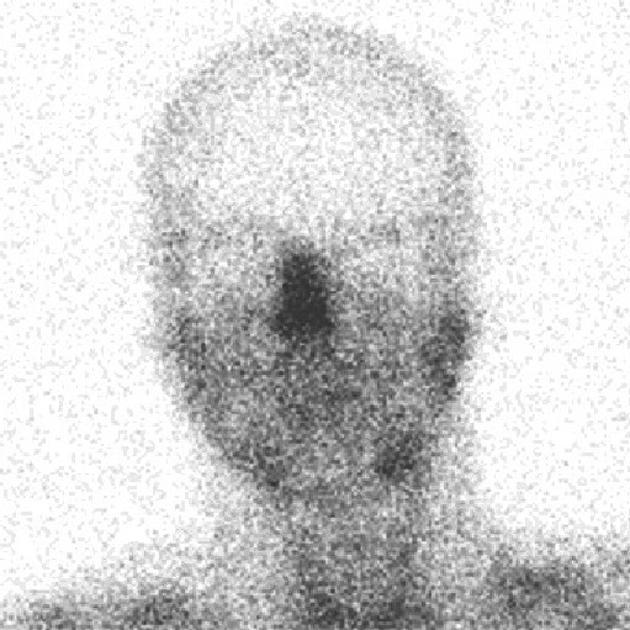
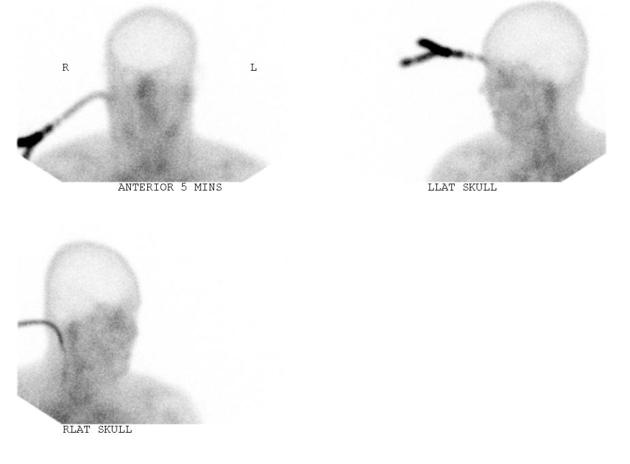
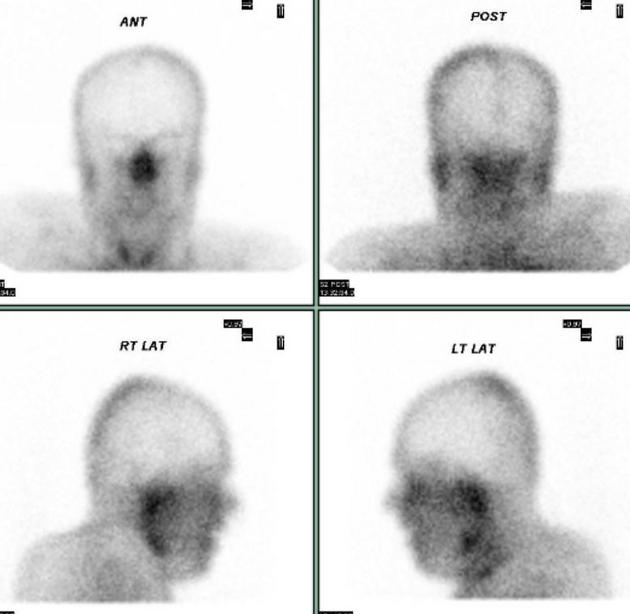
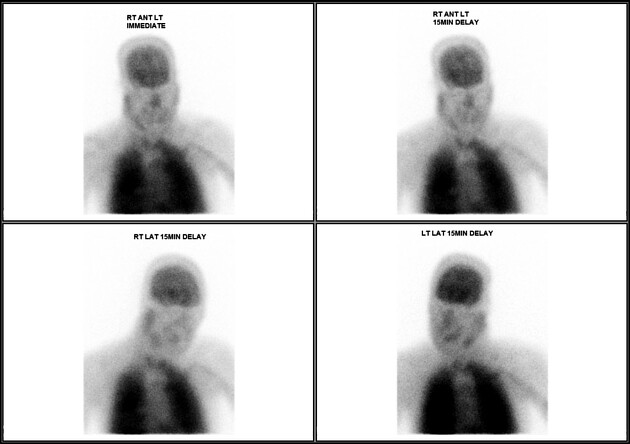
Nuclear medicine
Both radionuclide perfusion scintigraphy-SPECT and radionuclide angiography can be employed and have high sensitivity 4,13.
Cerebral perfusion
flow images are obtained in the anterior projection; delayed images follow 5 to 10 minutes after the injection
empty light bulb sign: absent intracranial uptake
hot nose sign: increased external carotid artery perfusion to the nasal region (an interesting sign, but of no real diagnostic value) 1









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.