
A brown tumor, also known as osteitis fibrosa cystica and rarely as osteoclastoma, is one of the manifestations of hyperparathyroidism. It represents a reparative cellular process, rather than a neoplastic process. Histologically brown tumors are identical to giant cell tumors (both are osteoclastomas), and therefore, this entity can easily be misdiagnosed as such if elevated blood calcium and/or parathyroid hormone levels are not assessed for and identified. Their name is derived from the brown coloration of the tumor macroscopically.
On this page:
Epidemiology
Brown tumors have a slightly greater frequency in primary than in secondary hyperparathyroidism (3% versus 2%). However, secondary hyperparathyroidism is much more common than primary hyperparathyroidism, therefore most brown tumors that are seen are associated with secondary hyperparathyroidism.
Pathology
In chronic renal disease, continual and excessive urinary calcium excretion can lower serum calcium level and lead to a rise in parathyroid hormone secretion. This results in mobilization of skeletal calcium through rapid osteoclastic turnover of bone to maintain normal serum calcium levels.
In localized regions where bone loss is particularly rapid, hemorrhage, and reparative granulation tissue, with active, vascular, proliferating fibrous tissue may replace the normal marrow contents, resulting in a brown tumor.
Hemosiderin imparts the brown color (hence the name of the lesions), and these are not eponymous, hence the word 'brown' should not be capitalized.
It is worth noting that the 2020 edition of Robbins & Cotran Pathologic Basis of Disease states that a "brown tumor" is a mass lesion which results from fibrous tissue ingrowth, whereas osteitis fibrosa cystica is the combination of cystic brown tumors, peritrabecular fibrosis and increased bone activity 5. It seems that most of the literature does not make a distinction between these two entities.
Location
Common sites of involvement include 4:
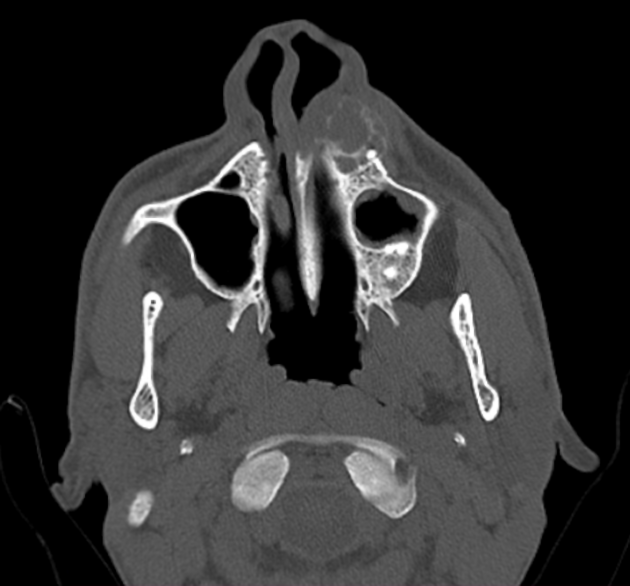
mandible
clavicle
ribs
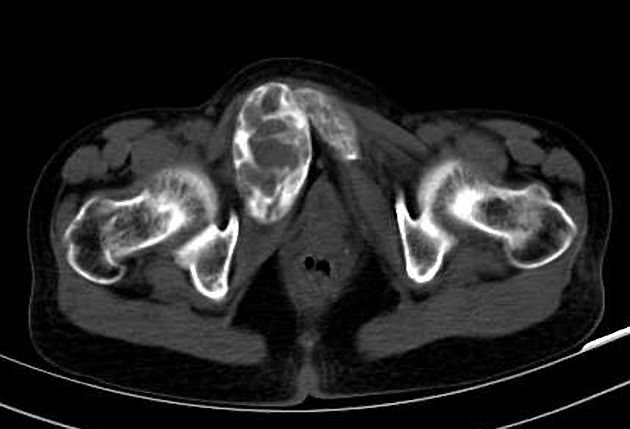
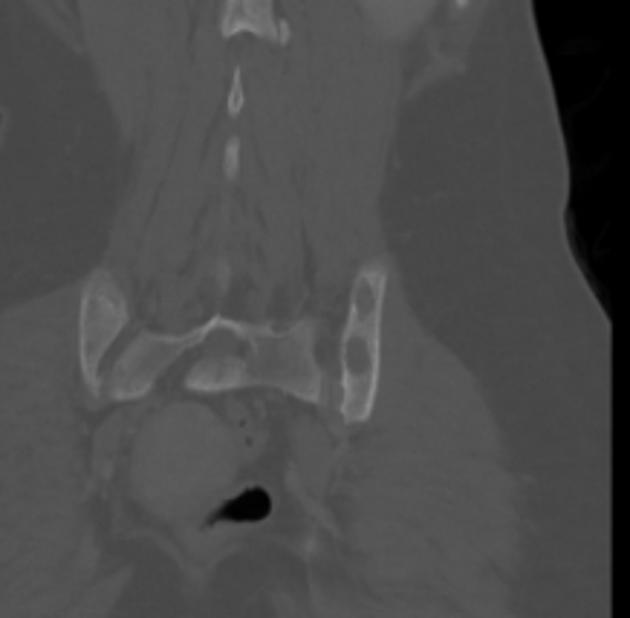
pelvis
Radiographic features
Plain radiograph
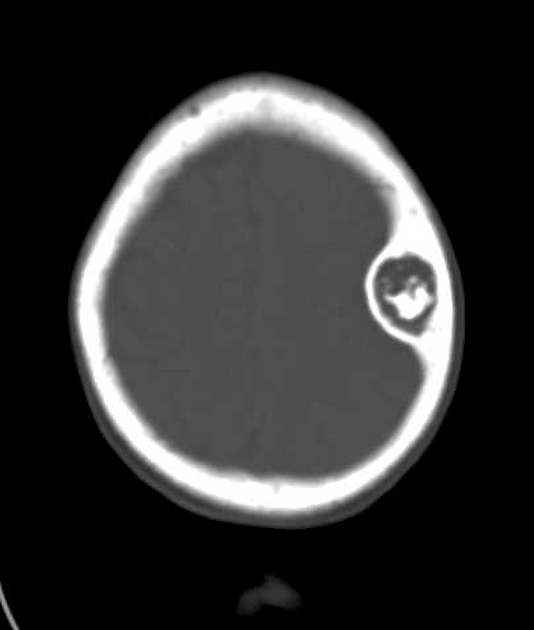
Well-defined, purely lytic lesions that provoke little reactive bone. The cortex may be thinned or expanded, but will not be penetrated.
CT
Attenuation values on CT will be in the range of blood and fibrous tissue.
Angiography (DSA)
Lesions are usually hypervascular.
MRI
The MRI appearance depends on the relative proportion of its components. The lesions, therefore, may be solid, cystic, or mixed. Solid components are intermediate to low intensity on T1- and T2-weighted images, while the cystic components are hyperintense on T2-weighted images and may have fluid-fluid levels.
T1 C+ (Gd): there can be enhancement of the solid component and septa
Nuclear medicine
Bone scan often shows intense uptake.
Treatment and prognosis
Brown tumors are typically treated by management of the underlying endocrine disorder of hyperparathyroidism. In cases where there is a pathological fracture or impending fracture, surgical fixation may be indicated 6.
Differential diagnosis
mnemonic for the differential diagnosis of a lucent/lytic bone lesion: FEGNOMASHIC











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.