
Cholescintigraphy is the use of radiotracers to assess the anatomy and function of the biliary system (and the liver indirectly). This is most commonly performed with Tc-99m-IDA analogs 1, and "hepatic IDA" imaging gave rise to the more common term "HIDA scan."
Indications
Cholescintigraphy can be used for the evaluation of 1:
-
the most common use is to confirm acute cholecystitis after an equivocal ultrasound study
if the tracer does not enter the gallbladder after a sufficient length of time, then this is compatible with obstruction of the cystic duct
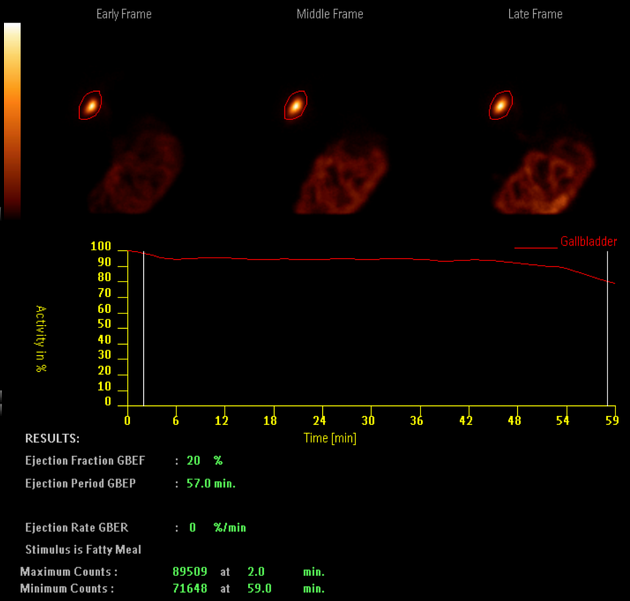
chronic cholecystitis: diagnosed if an adequate percentage of bile mixed with radiotracer does not exit the gallbladder after administration of cholecystokinin (CCK)
biliary atresia in neonates: good hepatic uptake of the tracer with no evidence of excretion into the bowel at 24 hours
bile leak: if tracer spreads outside the biliary system, it provides direct evidence of a biliary leak
biliary obstruction: tracer dose is held up before it can progress into the duodenum
confirmation of biliary dilatation: may be useful in imaging choledochal cysts
sphincter of Oddi dysfunction
With the exception of biliary atresia (and possibly chronic cholecystitis), cholescintigraphy is rarely a first-line imaging modality but is often used as a problem-solving tool.
Technique
Patient should be fasted for 4-6 hours before commencement of the exam. Infants should be given phenobarbital orally at 5 mg/kg/day for 3-5 days before the exam to increase hepatic excretion of the radiopharmaceutical during the investigation of biliary atresia 1. The steps are as follows 1:
the patient lies supine with the gamma camera located in front of the patient
the radiopharmaceutical is injected intravenously; after intravenous injection, IDA radiotracers are taken up by hepatocytes and then excreted into the biliary system 1
at 45 minutes after the injection, one-minute 128 x 128 dynamic images are acquired; this is the time when the gallbladder is well distended and easily imaged
a liquid fatty meal such as 300 mL of full cream milk is given to stimulate gallbladder contraction which excretes radiopharmaceuticals into the duodenum; images are taken for a further 45 minutes where the ejection fraction of the gallbladder can be calculated
if there is reflux of radiopharmaceuticals into the stomach, 100-200 mL of water can be given to dilute the radiopharmaceuticals
4 minutes before the end of imaging, 100 mL of water containing Tc-99m pertechnetate is given to delineate the stomach
-
if there are no radiopharmaceuticals within the bowels after 4-6 hours, biliary atresia should be suspected and a 24-hour image should be taken




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.