
Endometrioid carcinomas of the ovary are a subtype of epithelial ovarian tumors. The vast majority are malignant and invasive. On imaging, they are usually characterized as complex, non-specific solid-cystic masses and are associated with endometriosis.
On this page:
Epidemiology
Endometrioid carcinomas account for ~10% (range 8-15%) of all ovarian carcinomas. They are considered the second most common malignant ovarian neoplasm 8.
Both endometrioid and clear cell carcinomas are frequently associated with endometriosis 9.
Associations
-
synchronous endometrial carcinoma or endometrial hyperplasia may be present in up to a third of cases
the endometrial abnormality is thought to represent an independent, primary lesion rather than metastatic disease
endometrioid carcinoma is the most common malignant neoplasm arising within an endometrioma, although overall, this is an uncommon occurrence
Pathology
The typical gross appearance of these tumors is similar to that of other epithelial lesions, with variable cystic and solid components 2. Occasionally, they may be completely solid.
Histologically, an endometrioid carcinoma is characterized by the appearance of tubular glands and bears a strong resemblance to the endometrium. Squamous differentiation can be present in more than a third of patients 8.
A benign endometrioid carcinoma is relatively uncommon, and when it is benign it tends to be an ovarian cystadenofibroma 3.
Location
Bilateral involvement can be seen in ~30% (range 25-40%) of cases 1,2,8.
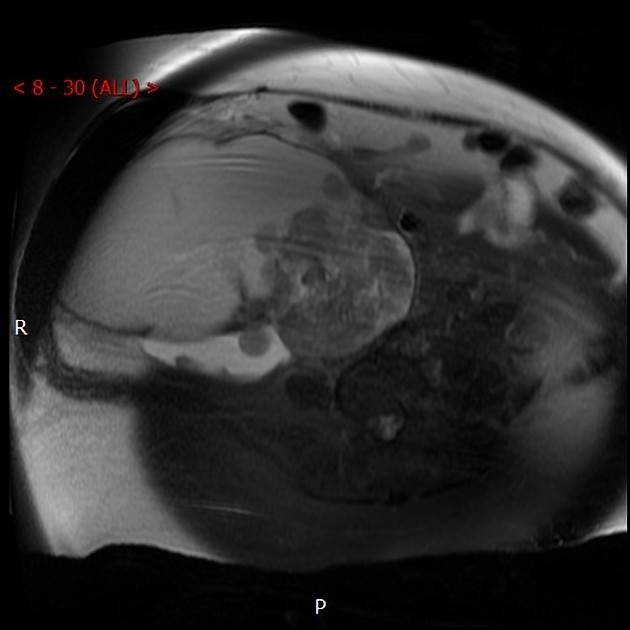
Radiographic features
Imaging findings are often non-specific and include a large, complex cystic mass with solid components. There may be associated endometrial thickening, evidence of endometriosis, or a contralateral mass.
MRI
Signal characteristics
-
T2
relatively low signal intensity of the tumor wall
shading sign may be seen 3
T1 C+ (Gd): can show mild enhancement 3
Treatment and prognosis
Endometrioid histology may carry a slightly better prognosis than a serous or mucinous cystadenocarcinoma of the ovary (not a serous tumor in general) independent of stage 5,8. Pure endometrioid tumors carry a far better outcome than a mixed variety.
Differential diagnosis
Metastases to the ovary with colon cancer could be considered especially if the ovarian lesion is bilateral or if there is a known colonic mass, especially due to strong histological similarity. Differentiation from metastatic endometrial cancer can also sometimes be difficult.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.