
Epiglottitis, also known as supraglottitis, is a life-threatening condition caused by inflammation of the epiglottis and aryepiglottic folds 1, which can lead to acute airway obstruction.
On this page:
Terminology
Supraglottitis refers to inflammation of the supraglottic larynx which can extend to the tonsils and tongue base.
Epidemiology
The disease used to predominate in children of 3 to 6 years, but this has changed since routine vaccination against Haemophilus influenzae type B (Hib) became available in the 1980s. Childhood vaccination has now been introduced in most countries.
Adults are more likely to have more widespread inflammation (supraglottitis), the most frequent cause is Streptococcus and the incidence may be increasing 7. Comorbidities such as diabetes and malignancy predispose to emphysematous supraglottitis 8.
Pathology
Etiology
Haemophilus influenzae type B used to be the most common responsible organism but group A beta-hemolytic Streptococci is now more common due to the effectiveness of Haemophilus influenzae type B vaccinations 4. Less common infections include Staphylococcus aureus, Neisseria meningitidis, TB and viruses.
Epiglottitis can be caused by direct extension of infection from other adjacent head and neck regions, such as dental infection, tonsillitis, laryngopyocele and skin cellulitis 5.
Non-infectious causes include:
sarcoidosis which usually spares the true vocal cords with their sparse lymphatic system 5
trauma
thermal injury
chemical irritation
recreational drugs
chemotherapy
radiotherapy
Clinical presentation
Sore throat and odynophagia are common presenting symptoms in adults and may be accompanied by an altered voice.
In children there may be rapid progression beginning with a sore throat and leading to difficulty swallowing and drooling. However, other presenting symptoms include:
fever
difficulty speaking
inspiratory stridor 1
severe dysphagia 1
Acute epiglottitis is potentially life threatening due to the risk of airway obstruction, particularly in children. The adult form tends to have a lower risk of airway obstruction due to the larger size of the adult airway and better tolerance of supraglottic edema 5.
Radiographic features
Plain radiograph
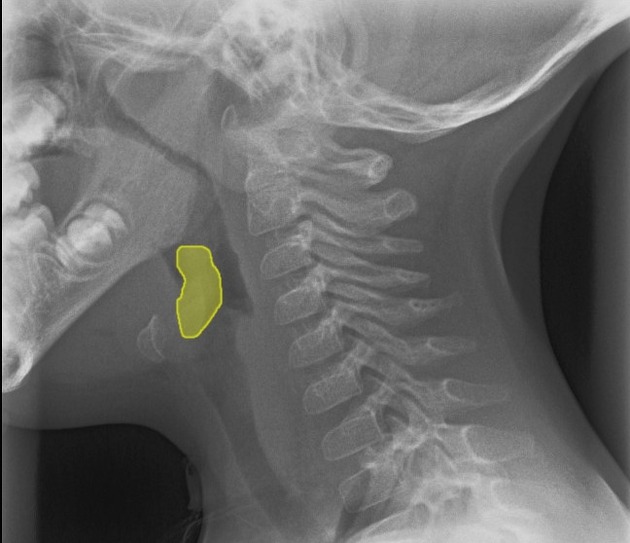
Lateral soft tissue radiograph of the neck demonstrates thickening of the epiglottis and aryepiglottic folds referred to as the thumb sign.
It should be noted that an omega epiglottis, either a variant of normal or in the setting of laryngomalacia, can result in a similar appearance and can be mistaken for epiglottitis.
In epiglottitis, the hypopharynx may be over-distended.
CT
CT is only rarely obtained, and usually when the diagnosis is unclear. Indeed, placing the child in the supine position can actually precipitate respiratory arrest. If a scan is obtained, marked edema and thickening of the epiglottis and aryepiglottic folds may be seen with narrowing of the airway.
Emphysematous infection may occur in adults and is accompanied by marked swelling.
Treatment and prognosis
Treatment must be expeditious given the life-threatening nature of the condition:
patients should be kept upright in a comfortable position
airway management with oxygen therapy
early tracheal intubation by specialist staff: if ET tube placement is impossible because of an inflamed epiglottis, emergency needle cricothyroidotomy may need to be performed
IV fluids
IV steroids and antibiotics
Differential diagnoses
-
croup (laryngotracheobronchitis)
subglottic narrowing and ballooning of hypopharynx
no epiglottis thickening
-
usually clinical following tonsillitis
-
asymmetric subglottic narrowing (intraluminal membranes)
all causes of epiglottic enlargement









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.