
An ileal conduit (or "Bricker conduit") was one of the original types of urinary diversions, and it is still in use today.
On this page:
Pathology
The conduit is most often placed after cystectomy (or cystoprostatectomy) for muscle-invasive bladder cancer. Although not a continent diversion, it may be preferred if the patient may have trouble self-catheterizing and maintaining a continent urinary diversion.
Procedure
The conduit is formed from 15-20 cm of distal but not terminal ileum that is isolated from the remainder of the ileum 5. The ureters are anastomosed to the proximal ileal segment and the distal segment is brought to the skin surface either as an end or loop stoma, usually in the right lower quadrant 5. The ileal loop continues to peristalse.
Complications
Complications can be divided into early (<30 days post-operative) and late (>30 days post-operative) 5:
-
early
- adynamic ileus, bowel obstruction, enteric anastomotic leak
- urine leak / urinoma
- urinary obstruction
- stoma retraction and/or necrosis
- urinary tract infection
- fluid collection / seroma
- enteric, cutaneous or genital fistula
-
late
- bowel obstruction
- ureteric and/or ureteroileal anastomotic stricture
- urinary obstruction
- ileal or stomal stenosis
- stomal retraction or prolapse
- parastomal hernia
- urinary tract infection
- urolithiasis
- tumor recurrence, e.g. in the upper urinary tract
- ureteroarterial fistula
Radiographic features
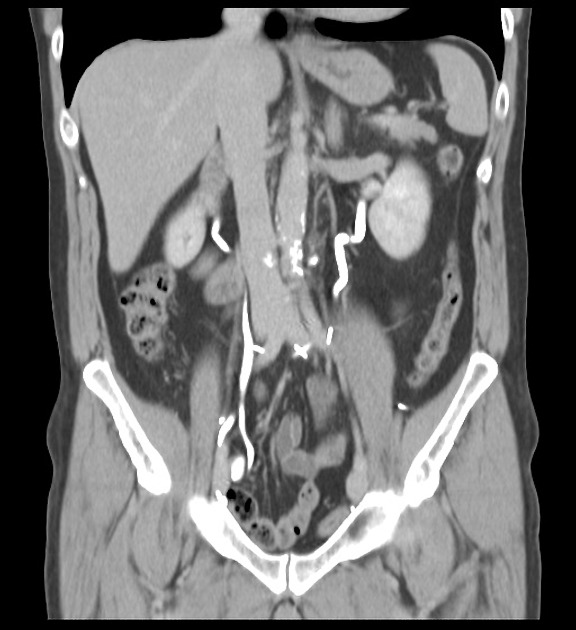
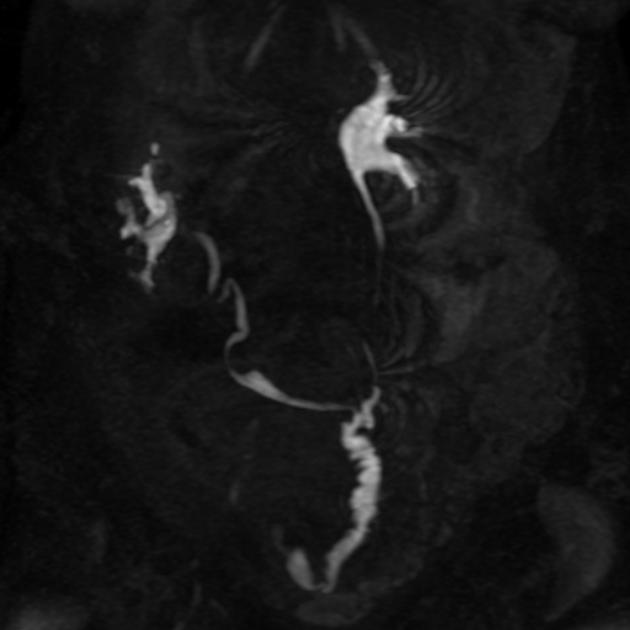
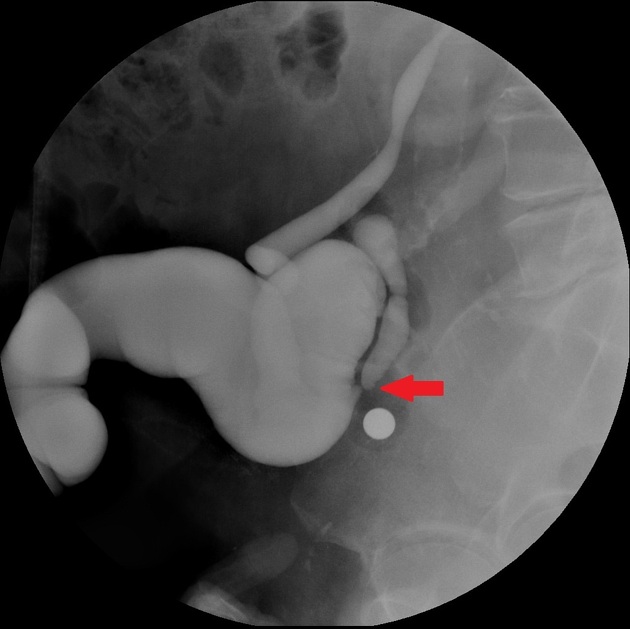
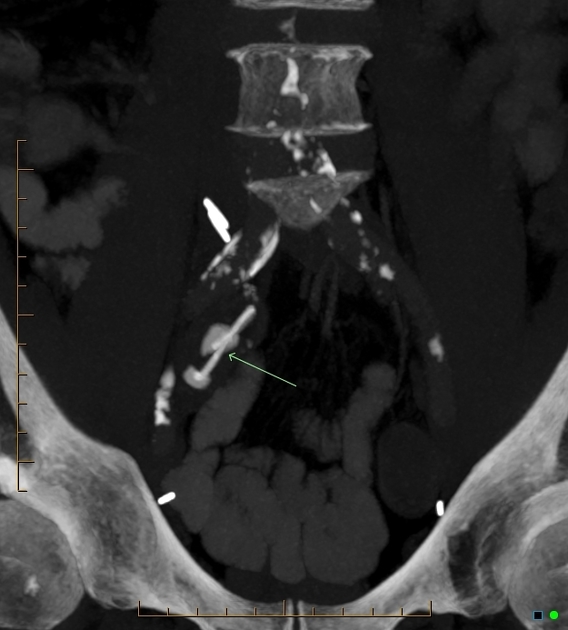
Ileal conduits are often imaged with CT urography (CTU) or through retrograde urography (loopogram). Both approaches have their benefits and disadvantages.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.