
Köhler disease is an eponymous term referring to childhood-onset osteonecrosis of the navicular in the foot. Müller-Weiss syndrome is the adult counterpart of navicular osteonecrosis 4,5.
On this page:
Epidemiology
Köhler disease typically presents in the pediatric population (4-6 years of age) and there is a recognized male predilection.
Pathology
Although the etiology remains unknown, a vascular incident is suspected. Delayed bone age has also been noted in some cases and may play a part in the pathogenesis of this entity. The central third of the navicular is a watershed area and it is prone more to avascular necrosis and stress fractures ref.
Radiographic features
Plain radiograph
the navicular may appear wafer-like (thinned) and fragmented
demonstrates patchy sclerosis (similar to osteonecrosis elsewhere)
often associated soft tissue swelling
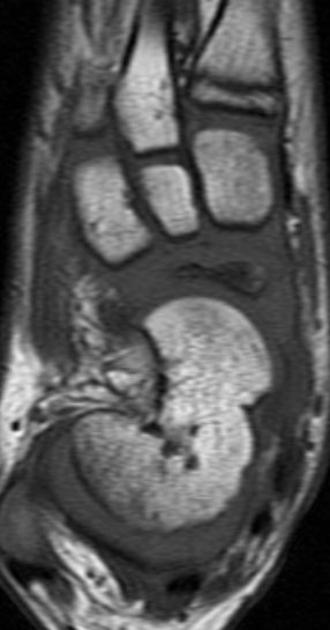
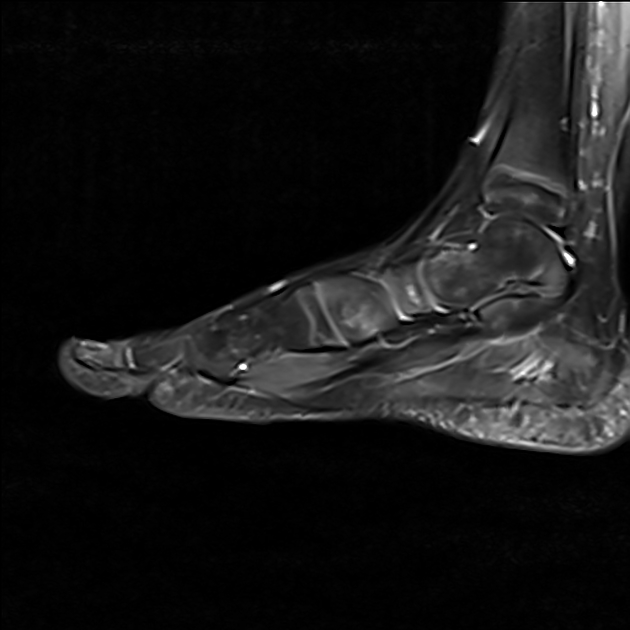
CT/MRI
Cross-sectional imaging is usually not required but may be necessary if pain persists or the diagnosis is not clear.
Treatment and prognosis
Köhler disease often tends to be self-limiting and heals spontaneously with re-ossification and reconstitution within a few years. Application of a below-knee weight-bearing cast may improve symptoms and is recommended, typically for 6-7 weeks.
History and etymology
It was first described in 1908 by Alban Köhler, a German radiologist (1874-1947) 1,6. Interestingly, the radiograph with which Köhler made his original case description is now not thought to be Köhler disease 7.
Differential diagnosis
Usually, there is little difficulty in making the diagnosis. If symptoms persist then findings of tarsal coalition should be sought. This can be misinterpreted as infection ref.












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.