
This is a basic article for medical students and other non-radiologists
Large bowel obstruction (LBO) occurs when there is mechanical obstruction of the large bowel and is often impressive on imaging on account of the ability of the large bowel to massively distend. This condition requires prompt diagnosis and treatment.
On this page:
Reference article
This is a summary article; read more in our article on large bowel obstruction.
Summary
-
epidemiology
- much less common than small bowel obstruction
- only 20% of all mechanical bowel obstruction
- epidemiology follows the underlying cause of obstruction
- colon cancer is the commonest cause 40-60% (typically sigmoid)
- much less common than small bowel obstruction
-
presentation
- cramp-like abdominal pain and distension
- constipation, nausea and vomiting
- dehydration and electrolyte imbalance may occur
- peritonism and shock may occur if there is any perforation
-
pathophysiology
- many causes of mechanical large bowel obstruction
- dilatation of proximal large bowel and collapse distally
- if dilated over 6 cm, the bowel wall may perforate
-
investigation
- plain films can be taken in patients with suspected obstruction
- may help to determine whether small or large bowel
- may help to determine the level of obstruction
- can be useful to diagnose volvulus
- CT is a much more helpful test
- determines the level of obstruction and often the cause
- more helpful to look for complications, e.g. perforation or ischemia
- plain films can be taken in patients with suspected obstruction
-
treatment
- fluid resuscitation and electrolyte correction
- NG tube in the vomiting patient
- treatment is dependant on the cause
- volvulus - tube-decompression
- malignancy - resection or stenting
- diverticular disease - medical management with antibiotics
-
prognosis
- prognosis very dependant on the cause
- treated early prognosis tends to be better
- mortality increases if there are complications, e.g. perforation
Role of imaging
- confirm diagnosis
- identify level (and possibly cause) of obstruction
- identify any complications
- plan treatment
Radiographic features
Plain radiograph
The large bowel has the ability to distend up to approximately 6 cm in diameter (see the 3-6-9 rule). Since the large bowel tends to sit peripherally in the abdomen, it may be possible to determine the level of obstruction.
Sigmoid volvulus will be seen as a distended loop of bowel rising out of the pelvis and may have a coffee-bean configuration. There will often be proximal dilatation of the large bowel.
An obstructing tumor may cause complete or incomplete obstruction and result in proximal dilatation of the large bowel from the site of disease.
Chest radiograph to check for free gas under the diaphragm is also a useful screen for bowel perforation.
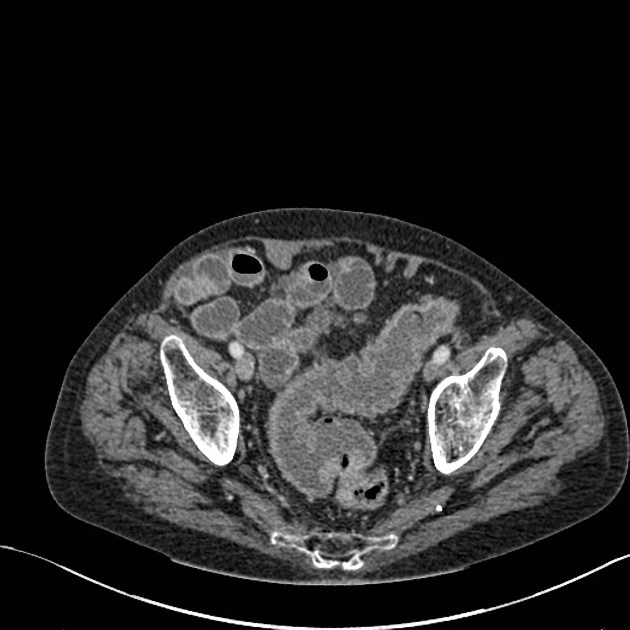
CT
CT scan of the abdomen is used to identify the site of obstruction, whether it is partial or complete and help identify the underlying cause.
The CT scan is almost always performed with IV contrast to delineate blood vessels and allow the enhancement of organs to be assessed. It is unusual to use oral contrast agents although some centers may continue to do so. Contrast enemas have also largely been replaced by CT.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.