
Meconium aspiration occurs secondary to intrapartum or intrauterine aspiration of meconium, usually in the setting of fetal distress, often in term or post-term infants.
On this page:
Epidemiology
Up to 10-15% of live births after 34 weeks can present with meconium stained fluid but only 1-5% of neonates develop meconium aspiration. There is no gender predilection.
Clinical presentation
There is commonly a history of meconium stained fluid at birth. Depending on the length of exposure, meconium skin staining may be present.
Neonates typically present with respiratory distress and varying degrees of hypoxia. Wheezing, hypercarbia and cyanosis may develop depending on the severity of the condition.
Pathology
Aspirated meconium can cause small airways obstruction and a chemical pneumonitis.
Radiographic features
Plain radiograph
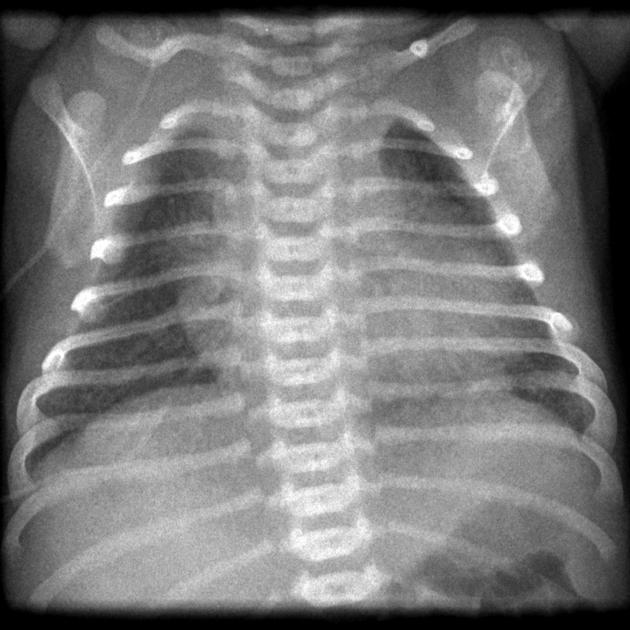
- increased lung volumes
- hyperinflated lungs with flattened hemidiaphragms
- secondary to distal small airway obstruction and gas trapping
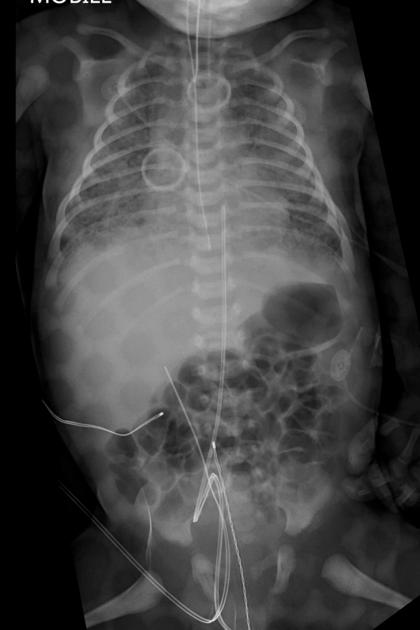
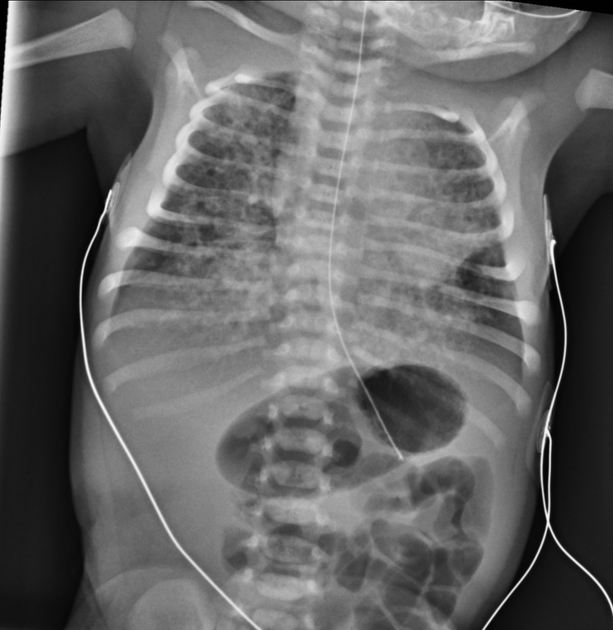
- asymmetric patchy pulmonary opacities
- due to subsegmental atelectasis
- may be 'rope like'
- pleural effusions can be seen
-
pneumothorax or pneumomediastinum in 20-40% of cases
- due to increased alveolar tension from obstructed airways
- multifocal consolidation
- due to chemical pneumonitis
Treatment and prognosis
Treatment usually involves suction of secretions and intubation and ventilation. Mortality can be as high as 10-20% in those with resulting severe pulmonary parenchymal disease.








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.