
Nephroblastomatosis refers to diffuse or multifocal involvement of the kidneys with nephrogenic rests (persistent metanephric blastema).
On this page:
Epidemiology
Nephrogenic rests are found incidentally in 1% of infants.
Pathology
If metanephric blastemas that persist beyond 36 weeks of gestation remain after four months of age, the lesions are called nephrogenic rests 3 and have the potential for malignant transformation into Wilms tumor.
It is believed that nephrogenic rests give rise to approximately 30-40% of Wilms tumors. Nephrogenic rests are found in up to 99% of bilateral Wilms tumors.
There are two pathologic subtypes of nephrogenic rest, perilobar rest (90%) and intralobar rest (10%), the latter more associated with Wilms tumor 2.
Intralobar rests are solitary and randomly distributed in the kidney, more centrally in the renal lobe. Perilobar rests are multiple and peripherally located in the kidney.
Associations
Intralobar:
Perilobar:
Radiographic features
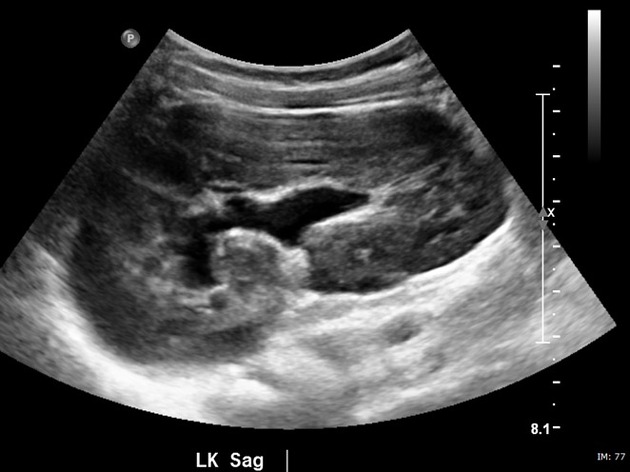
Ultrasound
Ultrasound may demonstrate hypoechoic nodules but is less sensitive than MR imaging and CT. Diffuse nephroblastomatosis is usually seen as reniform enlargement with a thick peripheral rind of tissue that may show striated enhancement. On ultrasound, the enlarged kidney may have diffusely decreased echogenicity.
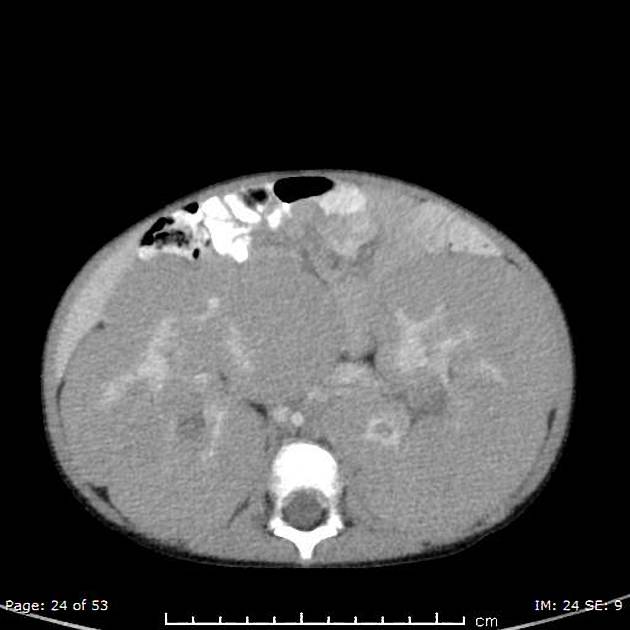
CT
At CT, macroscopic nephrogenic rests appear as low-attenuation peripheral nodules with poor enhancement relative to that of adjacent normal renal parenchyma.
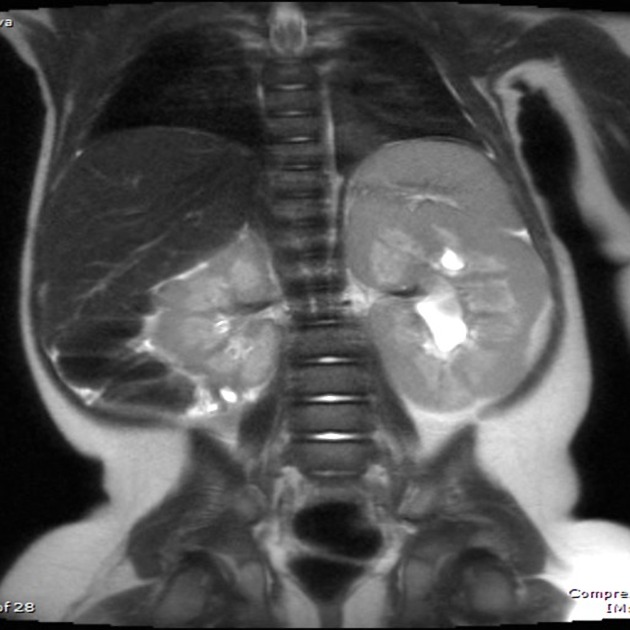
MRI
Typical signal characteristics include:
T1: the nodules demonstrate low-signal-intensity foci
T2: the nodules demonstrate low-signal-intensity foci
T1 C+ (Gd): hypointense mass enhances less than renal tissue
Treatment and prognosis
Treatment for nephrogenic rests is controversial. Some investigators recommend chemotherapy, whereas others maintain that close serial radiologic evaluation of enlarging masses is sufficient.
Differential diagnosis
renal lymphoma can mimic the appearance of nephroblastomatosis but is unusual in infants and young children.
leukemia 4, 5




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.