
Osteoarthritis
Updates to Article Attributes
Osteoarthritis (OA) is the most common form of arthritis, being widely prevalent with high morbidity and social cost.
Terminology
Some authors prefer the term osteoarthrosis instead of osteoarthritis as some authors do not believe in an inflammatory cause as might be suggested by the suffix "itis". To differentiate OA from its erosive osteoarthritis, which is a different clinical and radiological entity, the
Epidemiology
Osteoarthritis is common, affecting ~25% of adults 7.
Clinical presentation
Patients present with decreased function from joint pain, instability and stiffness 7,10. Many cases of radiological OA are asymptomatic and conversely clinically apparent OA may not manifest radiographic change 9,10.
Pathology
The pathogenesis and pathophysiology of OA are yet to be fully understood 7. Despite emphasis being placed on articular cartilage degeneration, the remainder of the joint is involved including bone remodelling, osteophyte formation, ligamentous laxity, periarticular muscle weakness and synovitis 8,10.
LocationDistribution
OA can affect both the axial and appendicular skeleton. The most common peripheral joints affected include ref:
Risk factors
Strong risk factors for developing OA include 7,10:
- obesity
- increasing age
- female sex (particularly between ages 50-80)
- family history
Classification
Osteoarthritis can be:
-
primary/idiopathic/typical
- absence of an antecedent insult
- strong genetic component with the disease primarily affecting middle-aged women 5
-
secondary/atypical
- abnormal mechanical forces (e.g. occupational stress, obesity)
- previous joint injury
-
post-traumatic osteoarthritis
- accounts for ~12% of all OA 11
- major cause in young adults 9
- prior surgery
- crystal deposition (e.g. gout, CPPD)
- haemochromatosis
-
post-traumatic osteoarthritis
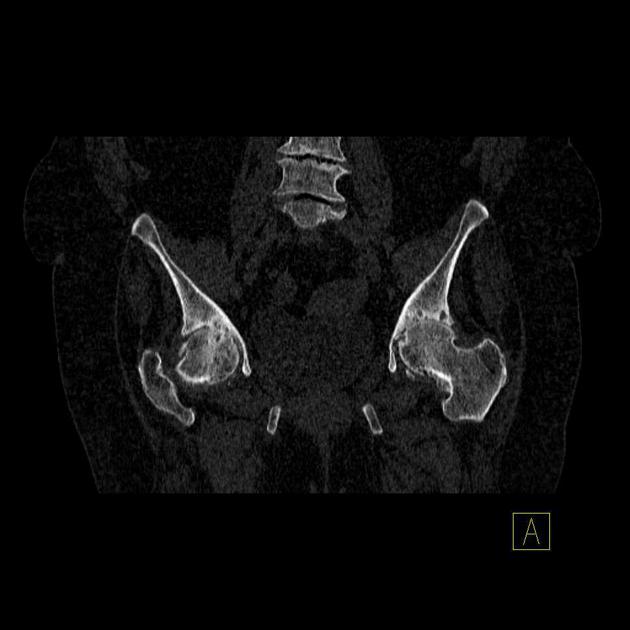
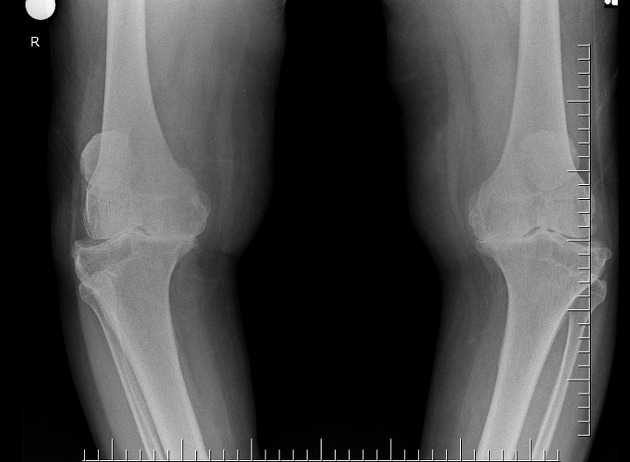
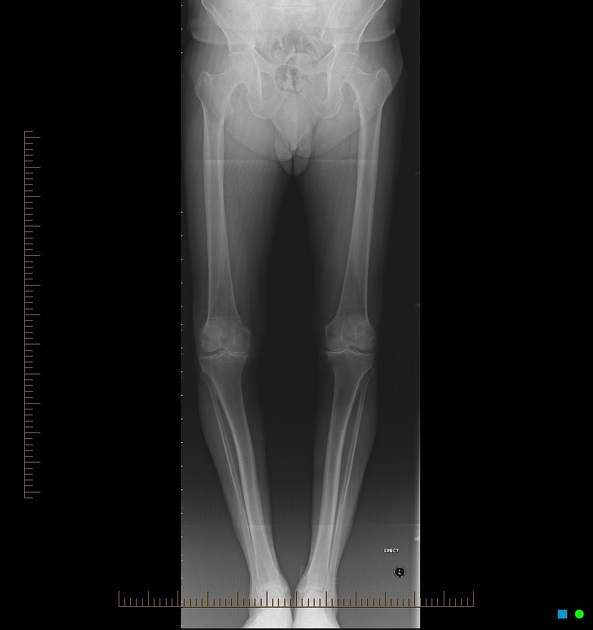
Radiographic features
Key radiographic features are joint space narrowing (JSN), sclerosis, and osteophytosis. If all three of these findings are not present, another diagnosis should be considered.
Joint space narrowing
- characteristically asymmetric
- least specific: present in many other pathological processes
Sclerosis
- sclerotic changes occur at joint margins
- frequently seen unless severe osteoporosis is present
Osteophytosis
- i.e. development of osteophytes
- common DJD finding
- will also be diminished in the setting of osteoporosis
- some osteophytes carry eponymous names, e.g. Heberden nodes, Bouchard nodes
Joint erosions
- several joints may exhibit degenerative erosions 1
- temporomandibular joint
- acromioclavicular joint
- sacroiliac joints
- symphysis pubis
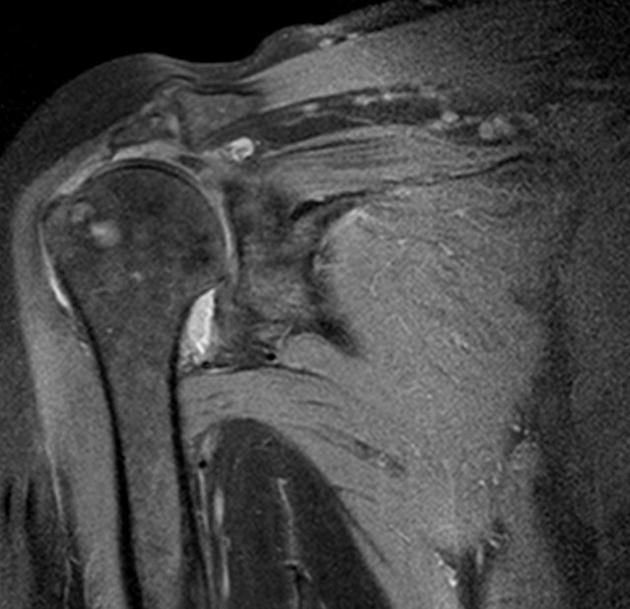
Subchondral cyst
- also known as a geode
- cystic formations that occur around joints in a variety of disorders, including, rheumatoid arthritis, calcium pyrophosphate dihydrate crystal deposition disease (CPPD) and avascular necrosis.
Treatment and prognosis
There is no effective treatment to slow or reverse the changes of osteoarthritis 7. The mainstays of treatment include exercise, walking aids, bracing, and analgesia (including intra-articular steroid injections) 8. Arthroplasty can result in improved function and reduced pain 10.
There is increasing evidence that the condition erosive osteoarthritis (EOA) is a severe form of 'normal' osteoarthritis and not a discrete disease entity and that therefore a subset of patients may progress from the non-erosive to the erosive form 6.











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.