
Subcutaneous emphysema (synonymous with the less common term surgical emphysema) refers to gas in the soft tissues. Gas is rarely limited to the subcutaneous layer and usually dissects into the deeper soft tissues and musculature along fascial planes.
On this page:
Clinical presentation
Clinically it is felt as crepitus and, if extensive, may cause soft tissue swelling and discomfort and restriction of movement. Subcutaneous emphysema is typically benign but can cause airway compromise, respiratory (ventilatory) failure, pacemaker malfunction and tension phenomena.
In the trauma situation the presence of gas indicates potentially serious injuries that require urgent management. Gas can track along fascial planes and enter the head, neck, limbs, chest, abdomen, and scrotum.
Pathology
Causes of subcutaneous emphysema can be divided into:
-
gas arising internally
perforated hollow viscus in the neck, e.g. esophageal perforation
-
gas introduced externally
penetrating trauma
-
iatrogenic
post-surgical
post-percutaneous intervention, e.g. pleural drain insertion
-
gas produced de novo
gas-producing infection(s), e.g necrotizing fasciitis
Trauma is the most common cause 5. Progression of subcutaneous emphysema following thoracic surgery should raise the suspicion for a possible bronchial leak 10.
Radiographic features
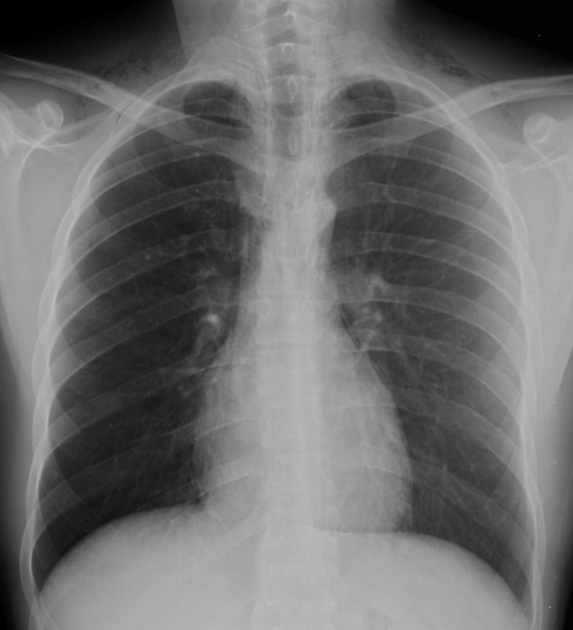
Plain radiograph
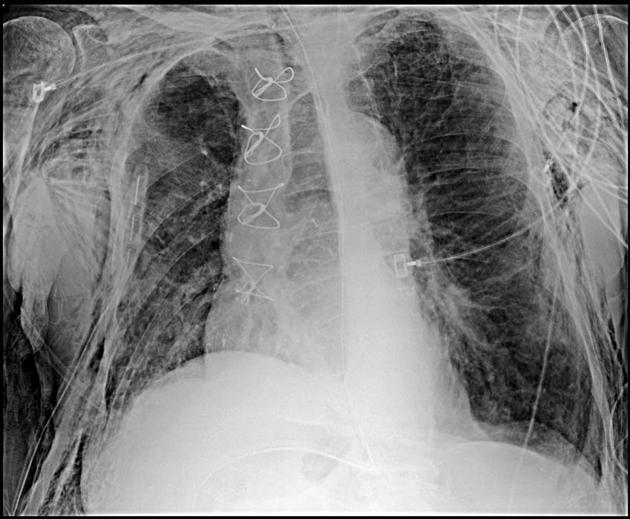
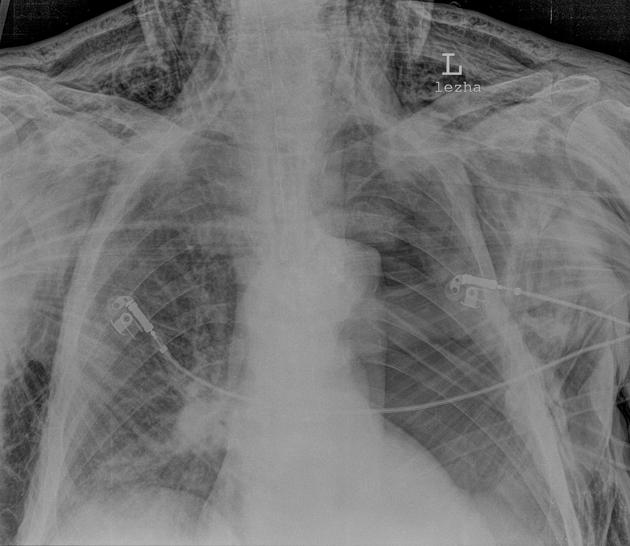
There are often striated lucencies in the soft tissues that may outline muscle fibers. If affecting the anterior chest wall, subcutaneous emphysema can outline the pectoralis major muscle, giving rise to the ginkgo leaf sign 2. Often there are displaced rib fractures indicating a cause of the gas.
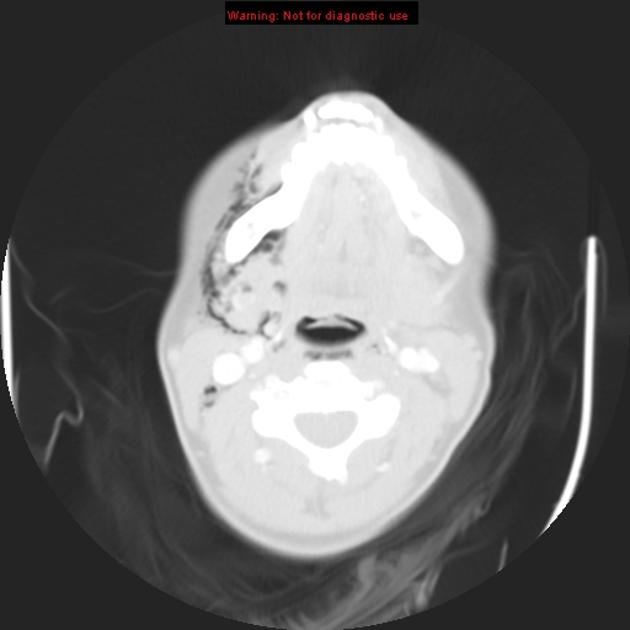
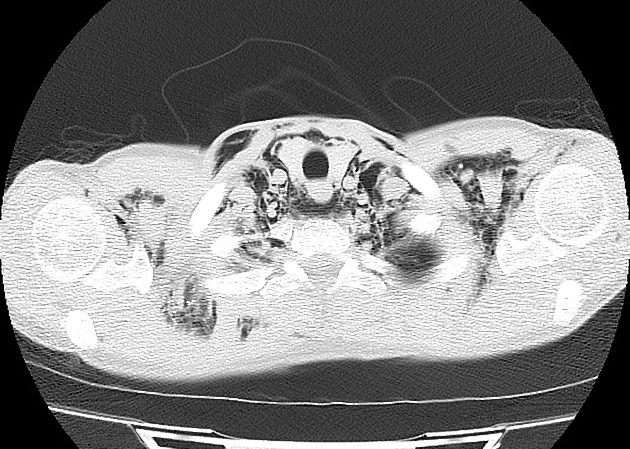
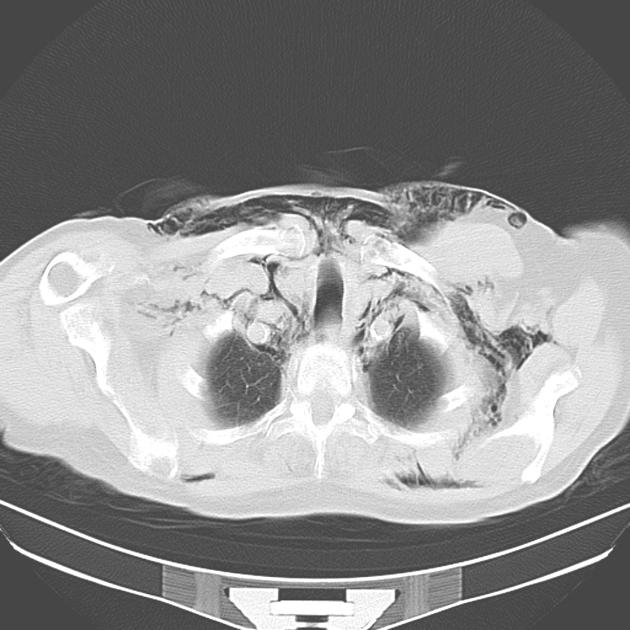
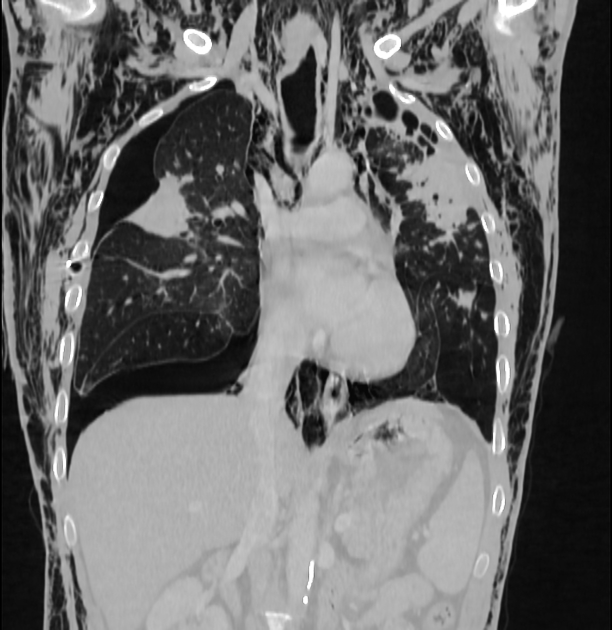
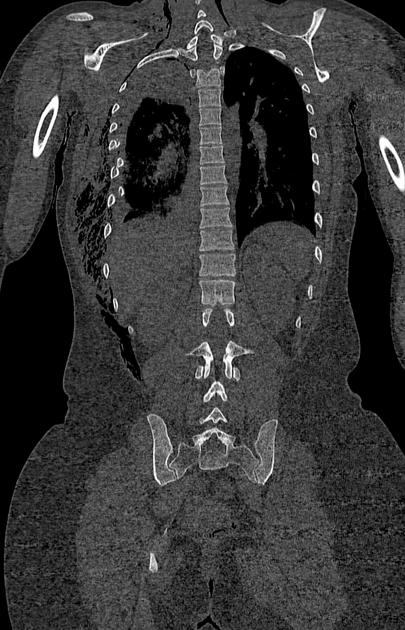
CT
Subcutaneous emphysema is readily visible on CT scans, with pockets of gas seen as extremely dark low (air) attenuation areas in the subcutaneous space.
Ultrasound
The mismatch in acoustic impedance between subcutaneous gas collections and surrounding soft tissue results in near-complete reflection of incident ultrasound waves, obscuring tissues in the far-field from the ("dirty") acoustic shadows cast by the hyperechoic, punctiform collections of gas. The scattering from the inhomogeneous collections will often result in reverberation and comet tail artifacts. Subcutaneous emphysema is particularly disruptive to lung ultrasonography, as it may obscure both normal structures and mimic other pathology 7;
-
well defined, anterior comet tail artifacts
extend indefinitely into the far-field similarly to B-lines
-
the artifacts cast from subcutaneous emphysema, however, do not originate from the pleural line and do not demonstrate respiratory dynamics
these artifacts are sometimes referred to as "E-lines" 8
-
static lung curtain sign
-
lateral and posterior subcutaneous emphysema may obscure the underlying lung and pleura
-
the descent of normally aerated lung with inspiration results in the temporary obscuration of the costophrenic recess and diaphragm
referred to as the "curtain sign" and is abrogated in the presence of a pleural effusion 9
-
-
the hyperechoic, linear collection of gas may be mistaken for the normal presence of a curtain sign
this may lead to the perhaps erroneous assumption that pleural effusion is absent
differentiated from the normal curtain sign by its lack of respiratory excursion
-
Treatment and prognosis
Treatment is directed at the underlying cause, while the subcutaneous gas is absorbed by the body over time. Symptomatic management should also be provided.
However, in rare instances where the subcutaneous gas is compromising overlying soft tissue, restricting ventilation or causing a compartment syndrome, gas can be released by the surgical division of the soft tissues or percutaneous drain insertion.













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.