
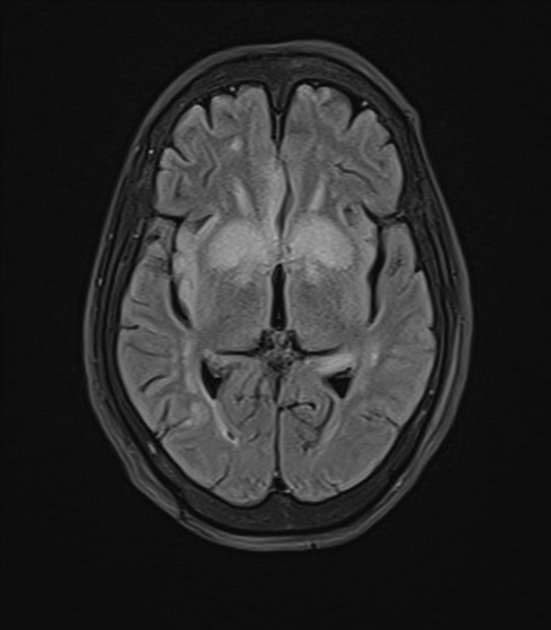
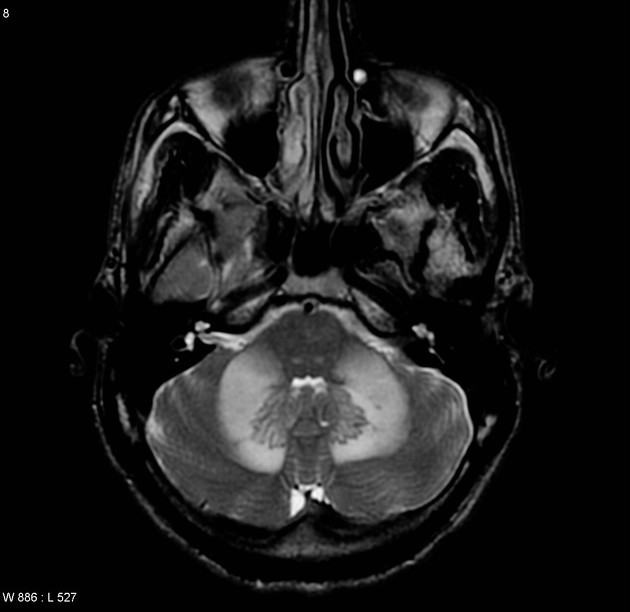
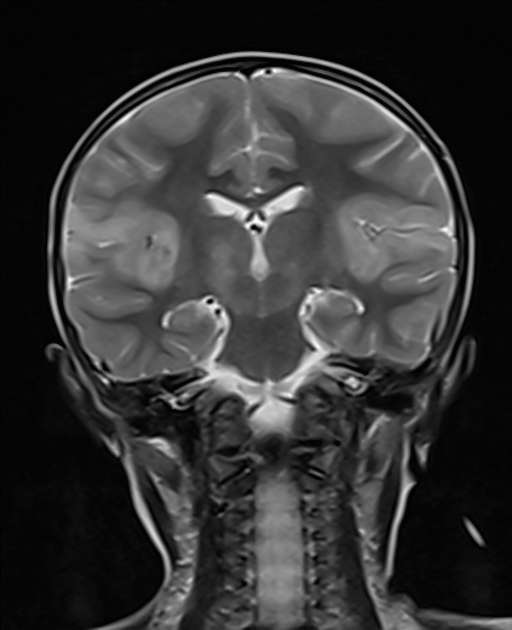
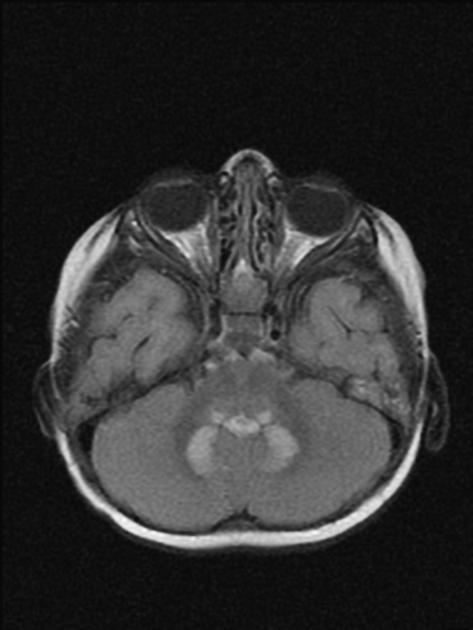
Symmetrical cerebral T2/FLAIR hyperintensities are seen in a broad range of pathologies. The differential depends essentially on the location of the lesions.
Symmetrical corticospinal tract lesions
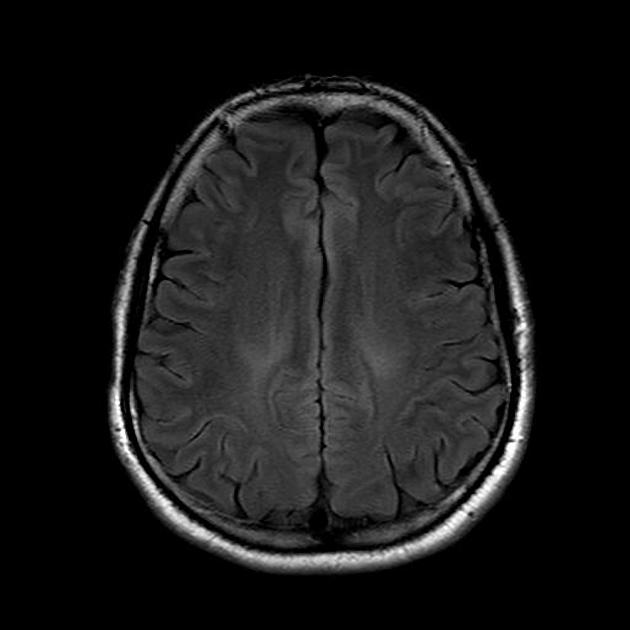
amyotrophic lateral sclerosis: symmetrical T2/FLAIR hyperintensities along the corticospinal tract from the cortices extending inferiorly to the brainstem and finally into the anterolateral column of the spinal cord
Symmetrical central tegmental tract lesions
central tegmental tract T2 hyperintensity : symmetrical hyperintensities of the extrapyramidal tract connecting the red nucleus and the inferior olivary nucleus 1
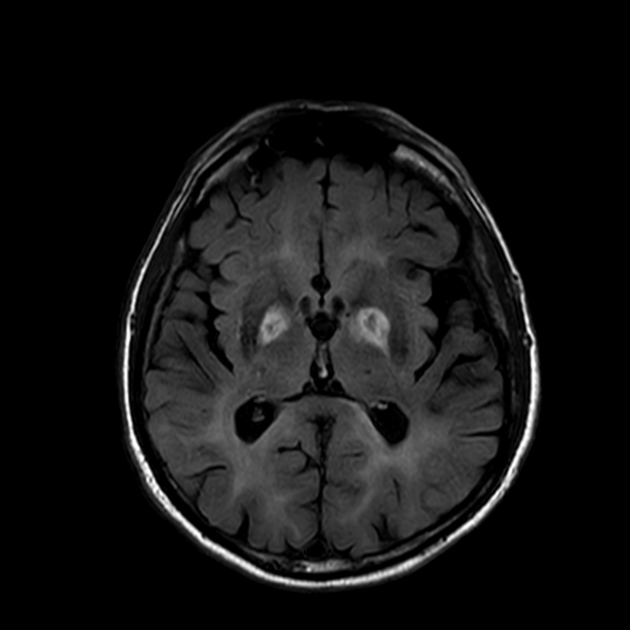
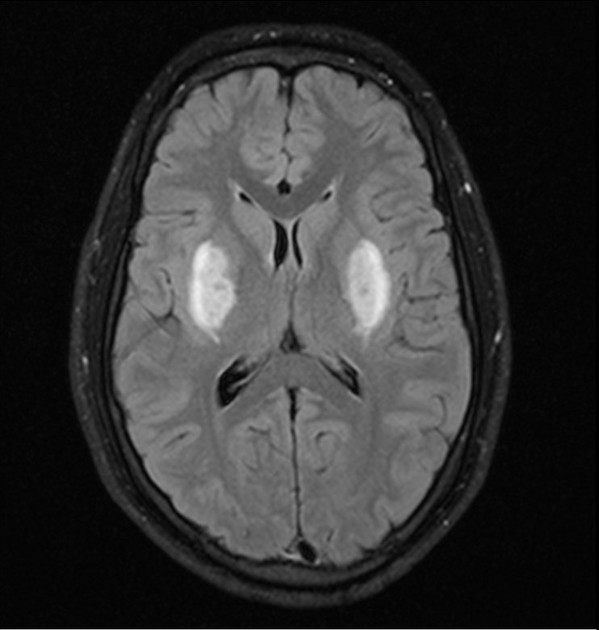
Symmetrical basal ganglia lesions
Leigh syndrome: distribution tends to be symmetrical in periaqueductal grey matter, medulla, brainstem, midbrain, putamen (not always present, but characteristic), globus pallidus, heads of the caudate nucleus, substantia nigra, subthalamic nuclei and thalami
carbon monoxide poisoning: globus pallidus is most commonly affected
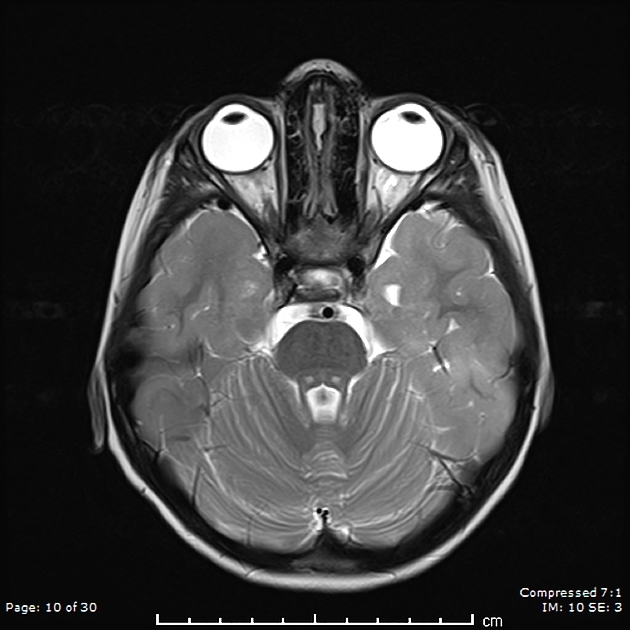
methanol poisoning: involves usually the putamen, optic nerves, and retina, but can also affect other basal ganglia nuclei, subcortical white matter, and cerebellum
cyanide poisoning: affects the basal ganglia, especially the striatum; the sensorimotor cortex may also be involved
organophosphate poisoning: affects putamen and caudate nuclei
ethylene glycol toxicity: basal ganglia and thalami, brainstem as well as amygdala and hippocampi
hypoglycemic encephalopathy: can involve the posterior limb of the internal capsule, cerebral cortex (specifically the insula and parieto-occipital), hippocampi, and/or basal ganglia
uremic encephalopathy: symmetrical lesions in the basal ganglia, thalamus, midbrain, and mesial temporal lobes
extrapontine myelinolysis: generally associated with central pontine myelinolysis, but can (rarely) be isolated, it shows symmetrical lesions in the basal ganglia, the internal, external, and extreme capsule
Wilson disease: involves basal ganglia (especially putamen), followed by midbrain, pons, and thalami 2
Symmetrical thalamic and mamillary bodies lesions
-
pulvinar sign: symmetrical bilateral T2/FLAIR hyperintensities involving the pulvinar thalamic nuclei
Wernicke encephalopathy: symmetrical lesions in mammillary bodies, dorsomedial thalami, tectal plate, periaqueductal grey matter, around the third ventricle
Symmetrical hippocampi lesions
Symmetrical pontine lesions
osmotic demyelination syndrome: located at the central portion of the pons
poliomyelitis-like syndrome: symmetric hyperintensities within the pons, substantia nigra, medulla, anterior horns of the spinal cord, and ventral nerve roots 3
LBSL: symmetrical lesions involving the posterior limbs of the internal capsules, the tracts of the trigeminal nerves, cerebellum, the dorsal columns and lateral corticospinal tracts of the medulla oblongata and spinal cord
Symmetrical middle cerebellar peduncle lesions
Please refer to our article on the middle cerebellar peduncle sign for the differentials of symmetrical lesions in this region.
Symmetrical temporal or insular lesions
hepatic encephalopathy: symmetric high signal within the insula, thalamus, and posterior limbs of the internal capsule, and cingulate gyrus
herpes simplex encephalitis: generally asymmetrical but symmetrical lesions may be seen 4
Symmetrical cerebellar lesions
Leigh syndrome: may involve the dentate nuclei, inferior cerebellar peduncles, periaqueductal grey matter, medulla, brainstem, midbrain, basal ganglia, substantia nigra, and thalami
heroin-induced leukoencephalopathy







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}