
Tennis leg represents a myofascial or tendinous injury of the lower limb and, not surprisingly, is seen most frequently in tennis players.
On this page:
Epidemiology
Although classically seen in people who play tennis, it can also be induced by playing squash, skiing, and athletics. Therefore, it typically occurs in active individuals, more frequently in middle-age. The same injury can also occur with more sedate activities, such as running to catch a bus. Extension of the knee and forced dorsiflexion of the ankle seem to be the most frequent biomechanical causes of the injury 2.
Clinical presentation
The presentation is one of sudden sharp pain in the posterior aspect of the calf, with a sensation of something 'snapping' within the calf 2. This is associated with focal tenderness and swelling, which can substantial. A focal gap can sometimes be felt early on (i.e. prior to swelling) at the site of the tear 1.
Pathology
Although tennis leg is fairly common, whether it represents a single entity or not is still debated. It involves injury to the muscles of the calf (superficial posterior compartment of the leg) via two identified mechanisms:
tear of the myotendinous junction of the medial head of the gastrocnemius
rupture of the plantaris tendon (thought to be an uncommon cause 2)
Both findings have been found in isolation or together.
Radiographic features
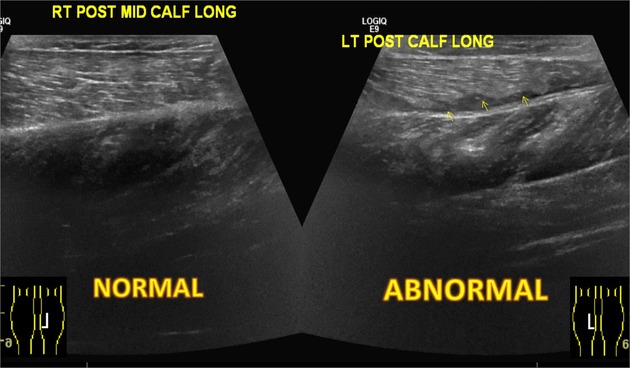
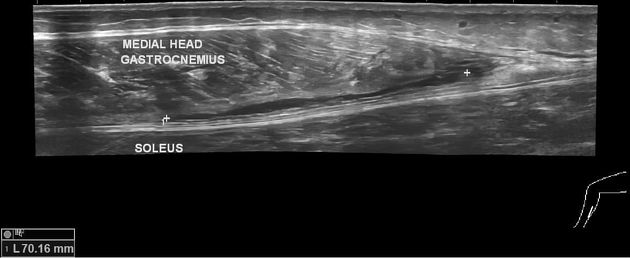
Ultrasound
Ultrasound demonstrates fluid deep to medial gastrocnemius and superficial to the soleus muscle, most prominent at the level of the myotendinous junction. A tear in the deep surface of gastrocnemius may be seen as a disruption in contour and echogenicity of muscle fibers. A torn plantaris tendon may also be identified.
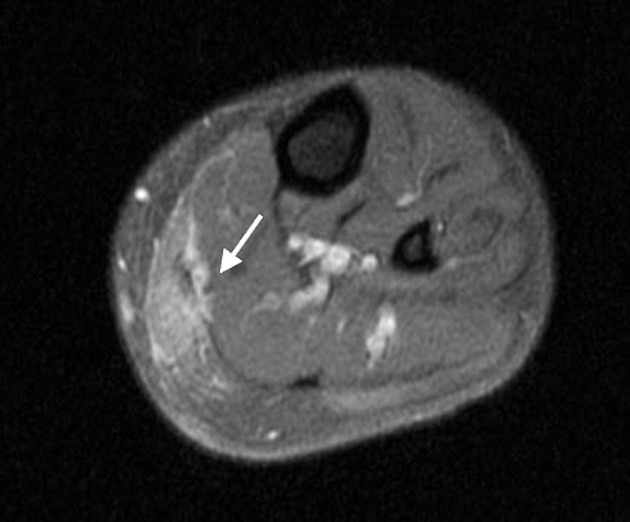
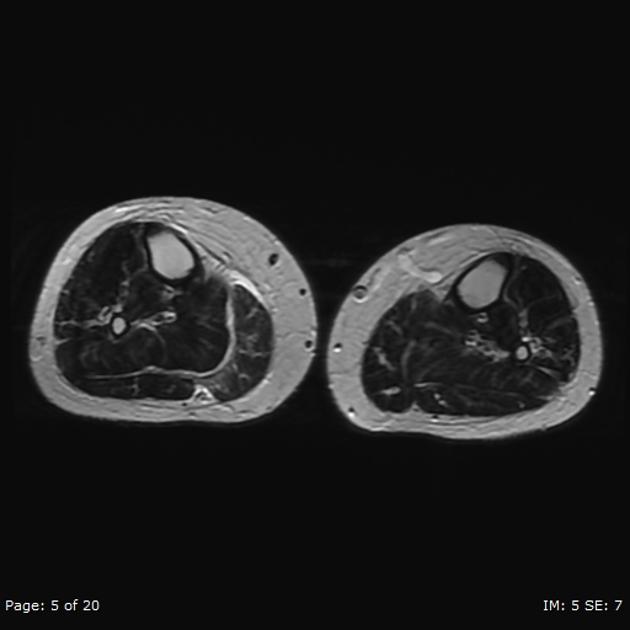
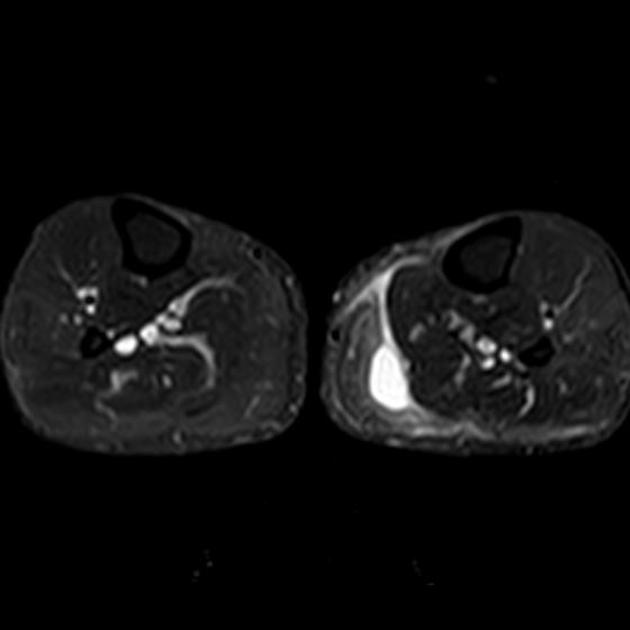
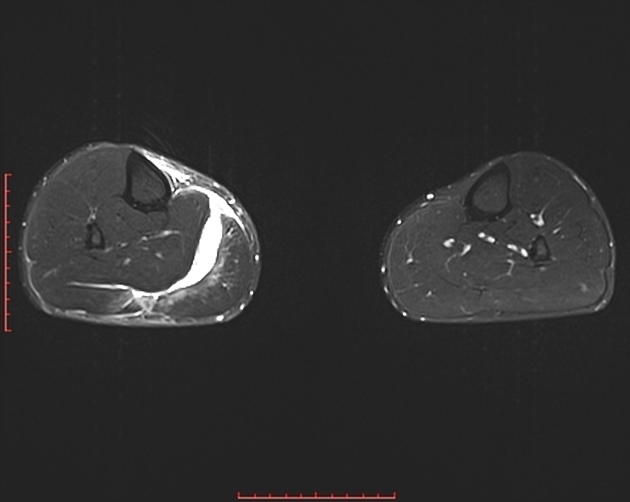
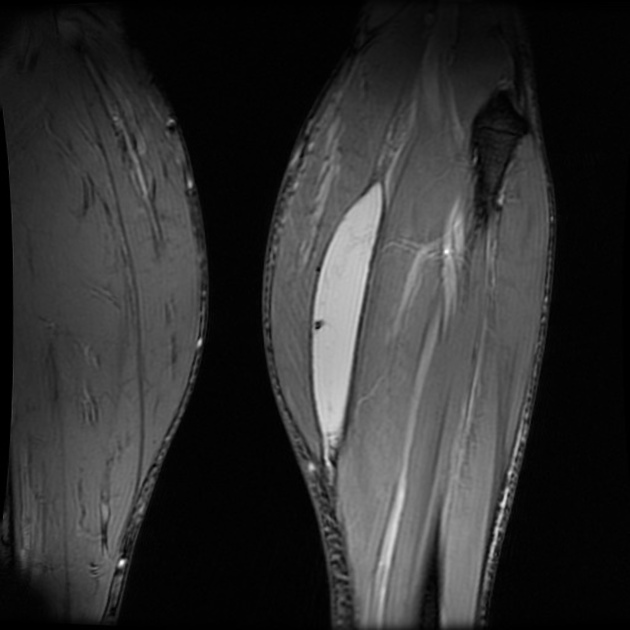
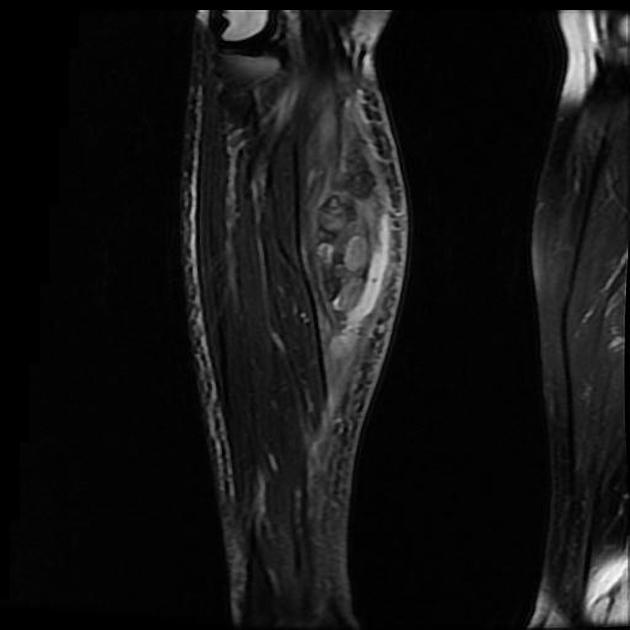
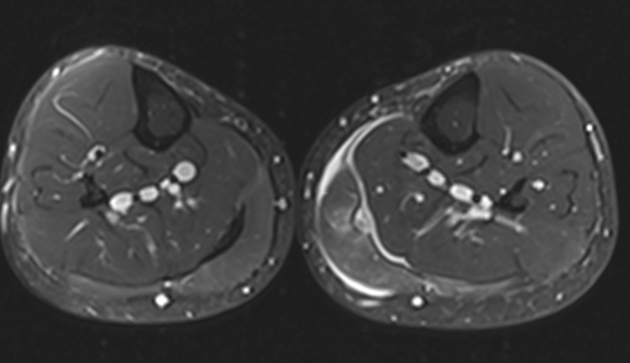
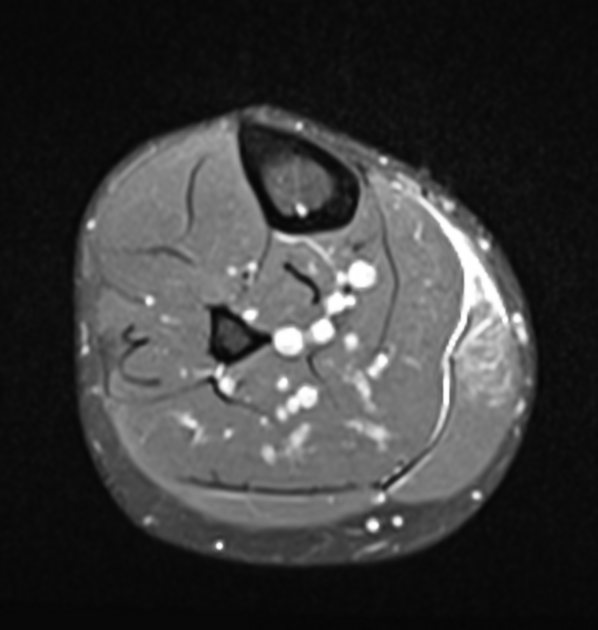
MRI
MRI demonstrates the same features seen on ultrasonography. Findings include:
high T2 signal fluid deep to medial gastrocnemius and superficial to the soleus
a focal area of disruption of muscle continuity noted along the deep aspect of the medial head of the gastrocnemius, with associated muscle edema
the plantaris tendon may either be torn or intact
Treatment and prognosis
Treatment is usually conservative as the condition is self-limiting. Only in cases where severe swelling leads to compartment syndrome is surgical fasciotomy necessary.
History and etymology
It was first described by R W Powell in 1883 2,3.
Differential diagnosis
On imaging consider:
deep vein thrombosis: may coexist with tennis leg
ruptured Baker cyst




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.