
Thymolipoma is a rare, benign anterior mediastinal mass of thymic origin, containing both thymic and mature adipose tissue.
On this page:
Epidemiology
Thymolipomas comprise ~5% (range 2-9%) of all thymic neoplasms, but are less common than a mediastinal lipoma of non-thymic origin. There is no recognized sex predilection and the reported age range is between 3-56 years, with a mean age of 22 years.
Associations
Unlike thymomas, thymolipomas are only occasionally associated with myasthenia gravis 1. In addition, they are also described in association with:
Clinical presentation
Most thymolipomas are asymptomatic and found incidentally, often due to imaging of respiratory tract infection 1. Symptoms, when present, are attributable to displacement of mediastinal structures. Approximately 25% complain of non-specific symptoms such as cough, dyspnea and chest pain, which may or may not be the result of the mass.
Pathology
Thymolipomas are composed of a mixture of mature adipose tissue with islands of thymic tissue. The etiology remains uncertain, with hypotheses proposed including 1:
true neoplasm of the thymus
variant of a thymoma
hyperplasia of mediastinal fat
neoplasm of mediastinal fat which engulfs thymic tissue
Irrespective of the cause, these tumors are slow-growing, only gradually increasing in size and are usually large at the time of diagnosis.
Location
They occur mostly in the cardiophrenic angles.
Radiographic features
A thymolipoma can grow to a very large size before discovery.
Plain radiograph
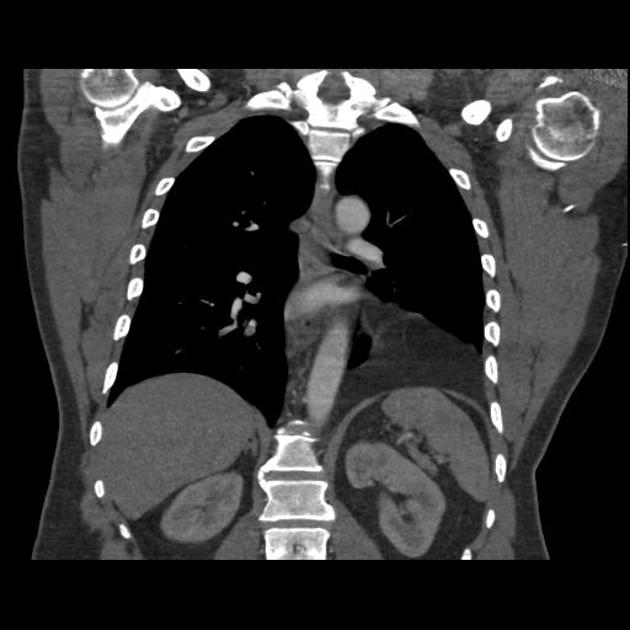
Typically these tumors appear as large anterior mediastinal masses. The larger tumors tend to hang down one or either side of the pericardium, and being soft, they mold themselves to the adjacent mediastinum and diaphragm and often mimic cardiomegaly 1. The predominantly fat density can be difficult to identify on plain radiographs, however, in larger masses that abut the diaphragm, the diaphragm can still be seen.
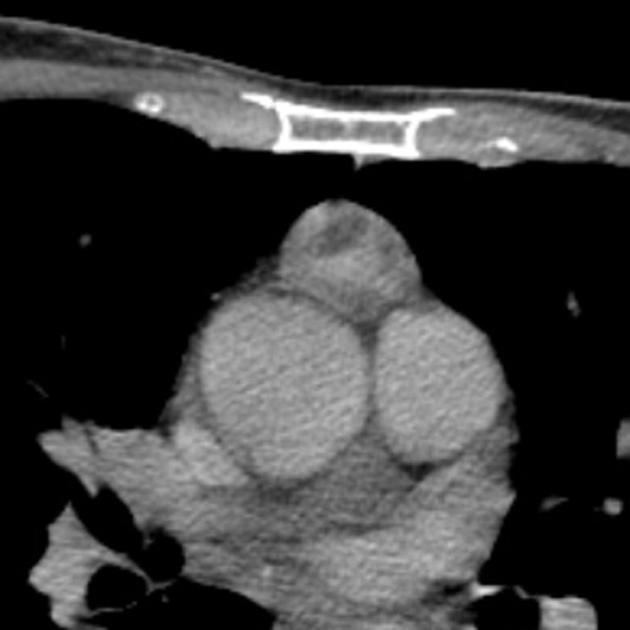
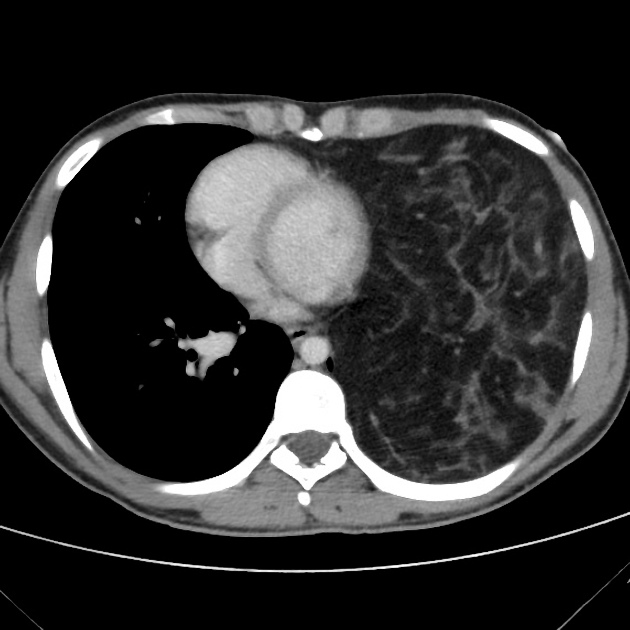
CT
On CT, thymolipomas typically appear almost entirely fatty with some areas of inhomogeneous soft tissue density that represent thymic tissue.
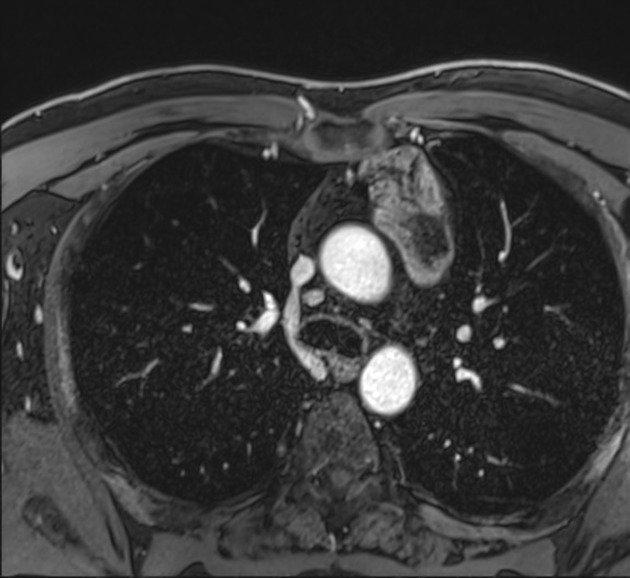
MRI
Thymolipomas have fat and soft tissue signal characteristics:
T1: typically the adipose tissue within the tumor is high T1 signal and the thymic component a more intermediate T1 signal
STIR/FS: shows complete suppression; consistent with subcutaneous fat
Treatment and prognosis
Surgical local resection is curative; there are no reports of recurrence, metastasis or mortality.
History and etymology
It was first reported by Lange in 1916. The term was coined by Hall in 1948.
Differential diagnosis
The differential on plain radiography is that of an anterior mediastinal mass. In larger tumors that "hang" down, causes of cardiomegaly should also be considered.
On CT the differential is much narrower and includes:
overgrowth of cardiophrenic fat pad
focal thymic hyperplasia: certain forms may have some imaging overlap in some situations



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.