
Airway foreign bodies in children are potentially fatal, which is why immediate recognition is important. Unfortunately, delayed diagnosis is common.
On this page:
Epidemiology
Children under the age of four years have an increased risk of foreign body (FB) aspiration, with a slight male predominance 1.
Clinical presentation
Most children (~70%) are witnessed to have had a choking event at the time of aspiration. Children may otherwise present with cough, dyspnea, or irritability 2,6.
Pathology
Most (70-90%) foreign bodies are organic, most commonly seeds and nuts. Inorganic foreign bodies vary dramatically and can include teeth, coins, pins, pens/crayons, etc.
Aspirated foreign bodies have a predilection for the right tracheobronchial tree, given the wider and steeper structure of the right main bronchus 6.
Radiographic features
The hallmark of an aspirated foreign body is a lung volume that does not change during the respiratory cycle 6. Medical imaging departments may have a dedicated suspected foreign body inhalation series.
Plain radiograph
-
the patient should be radiographed on expiration: this will exaggerate the differences between the lungs
in infants and toddlers, a parent can be asked to push inward and upward on the child's upper abdomen to encourage expiration
the normal lung should appear smaller and denser than the affected lung
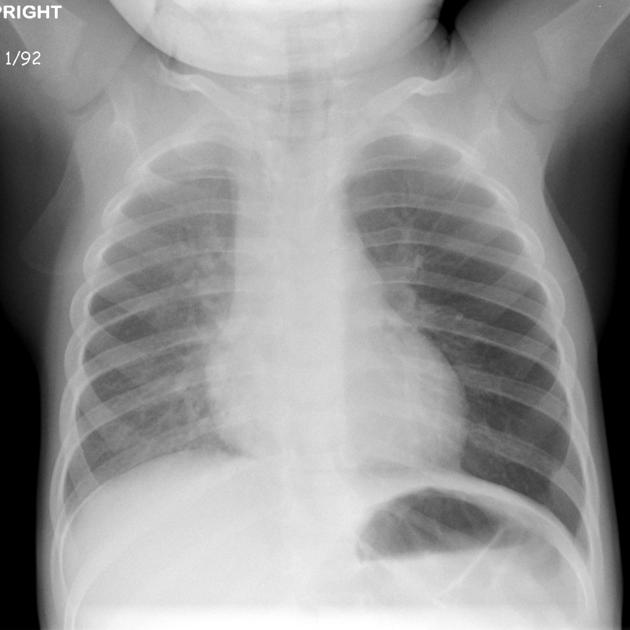
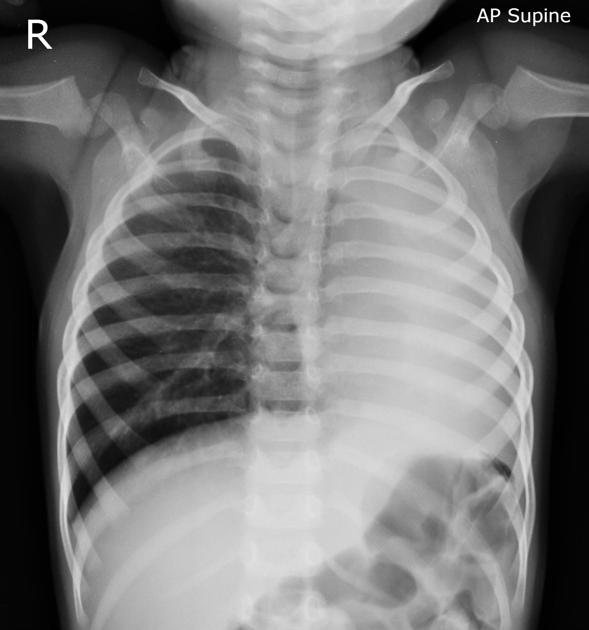
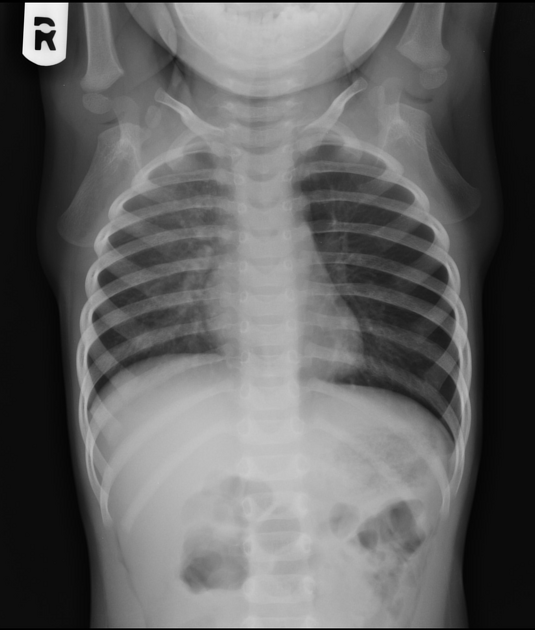
due to the check valve mechanism, air enters the bronchus around the foreign body but cannot exit, the affected lung will usually appear overinflated and hyperlucent, with concomitant rib flaring and a depressed ipsilateral hemidiaphragm
in uncooperative patients, bilateral decubitus views can be performed (case 1), which will demonstrate air trapping on the affected side 7. This view may increase false positives but not true positives and so its clinical value has been questioned 10
interrupted bronchus sign
the chest x-ray will be normal in ~35% (range 30-40%) of patients 1-2
the majority of foreign bodies are radiolucent 6
unilateral emphysema or atelectasis are the most common findings 1-2
Fluoroscopy
If the chest x-ray examination is inconclusive and there is ongoing high clinical suspicion of foreign body aspiration, fluoroscopy may be attempted. The child is imaged in the lateral decubitus position, lying on the presumed affected side. The occluded lung would be unchanged in volume and immobile through respiration.
CT
Can be performed at low dose to determine if bronchoscopy is needed and to identify the obstructed airway 8. As bronchoscopy often requires general anesthesia for children, it is important to avoid this procedure if it is not needed.
CT can also be useful in the assessment of a missed or retained foreign body after initial bronchoscopy 3.
Treatment and prognosis
Bronchoscopy is considered the gold standard in the diagnosis of tracheobronchial tree foreign bodies 3, with the added benefit of being able to potentially retrieve the foreign body.
Complications
Differential diagnosis
-
esophageal foreign body
flat foreign bodies (e.g. coins) tend to lie in the coronal plane in the esophagus 4
-
lung hyperinflation 6
asthma - usually bilateral
viral infection - usually bilateral
mass causing bronchial compression e.g. bronchogenic cyst, lymphadenopathy













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.