Colovesical fistulas are communications between the lumen of the colon and the bladder, either directly or via an intervening abscess cavity (foyer intermediaire). When the communication is between the rectum and urinary bladder, the term rectovesical fistula is used.
On this page:
Epidemiology
The demographics will match those of the underlying cause including 2:
diverticulitis: most common ~ 60%
colorectal cancer (CRC): ~ 20%
Crohn disease: ~ 10%
Clinical presentation
In most instances, the diagnosis is suspected clinically due to pneumaturia, faecaluria, recurrent urinary tract infections, or passage of urine rectally 4. In some cases, it will be first diagnosed radiologically at the time of investigation for the primary disease.
Radiographic features
The fistula usually occurs through the bladder dome (~ 60%). The posterior wall (~ 30%) and trigone (~ 10%) are less frequent sites 2. Colovesical fistulas and their causes can be characterized in several ways, although the fistulous tract itself is often difficult to demonstrate.
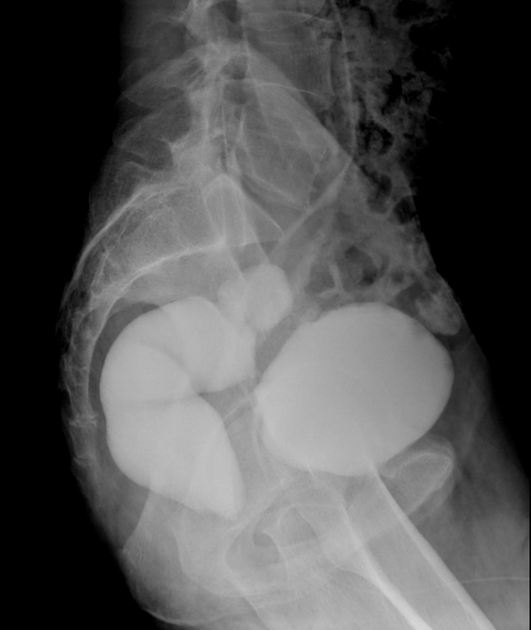
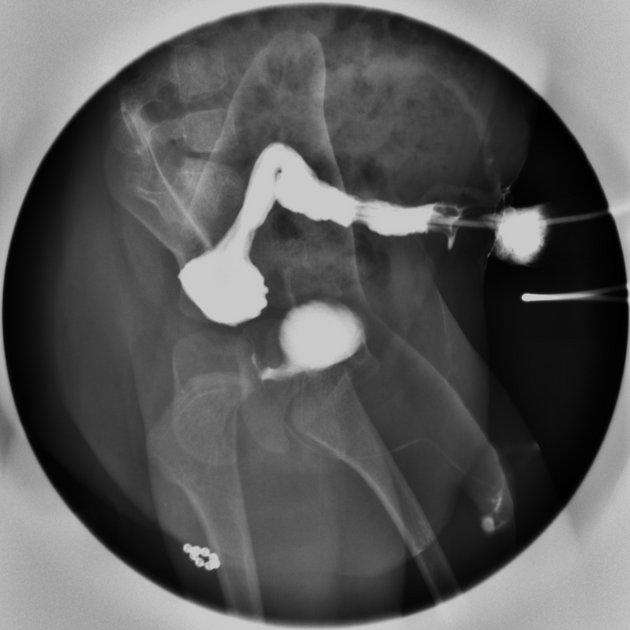
Fluoroscopy
A contrast enema is most likely to show the actual fistula, although this still occurs in a minority of cases. The underlying cause will be demonstrated, with relevant findings to the diagnosis (e.g. diverticula, stenosing mass lesion, changes of Crohn's disease).
The beehive on the bladder sign has been coined to describe the vesical end of the fistula as seen on the cystogram. It elevates the bladder outline in a rounded triangular fashion, reminiscent of a beehive 1.
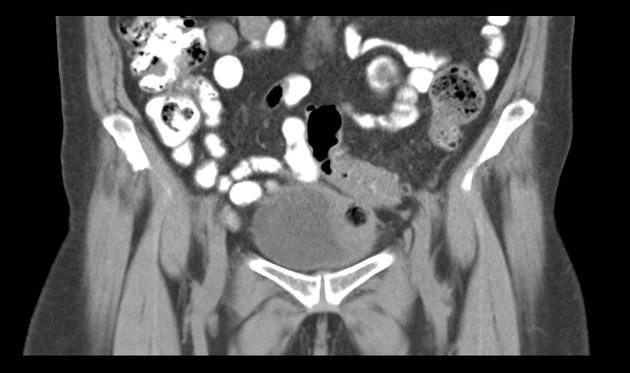
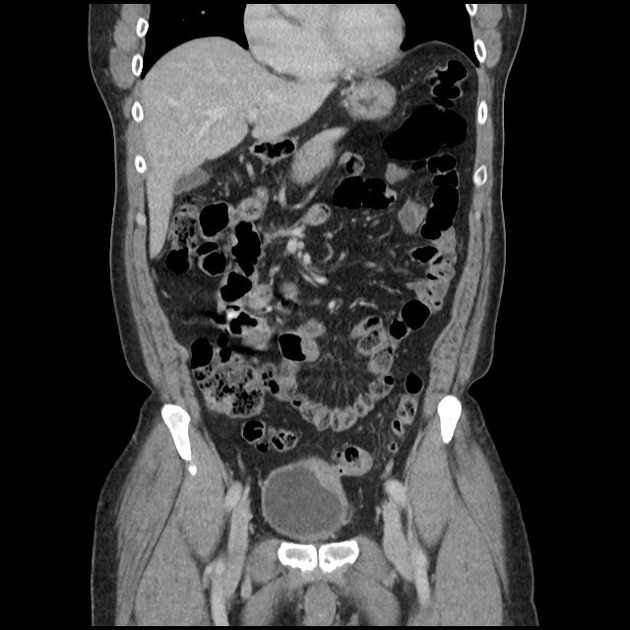
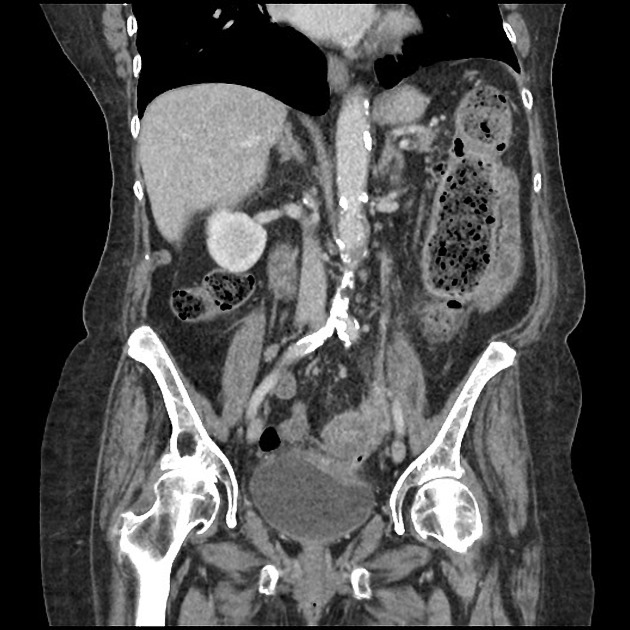
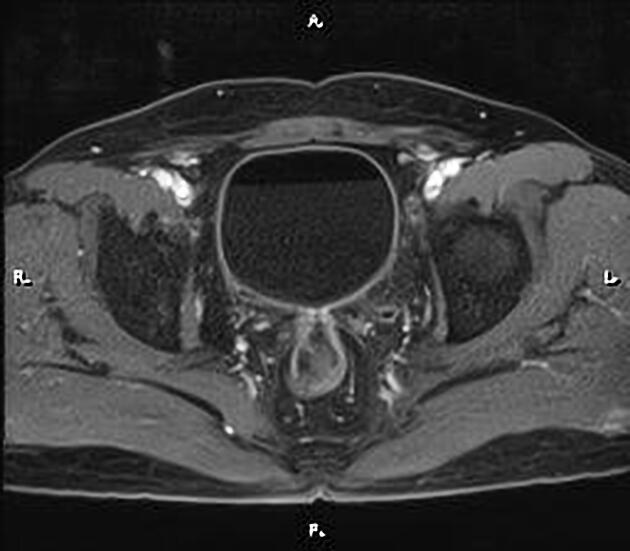
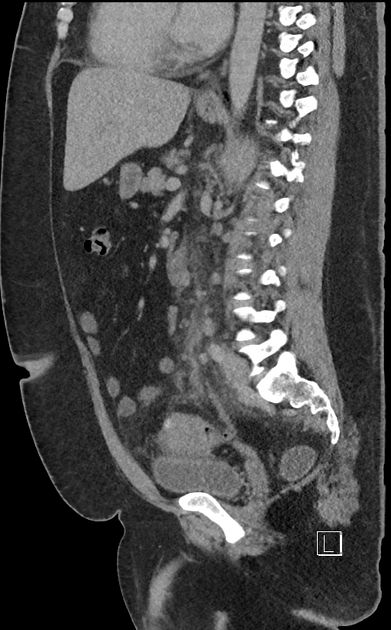
CT
On CT the fistula will be heralded by the presence of gas within the lumen of the bladder, or less frequently direct demonstration of the tract itself. Contrast may be instilled into the rectum 'on the table' before the acquisition of images to demonstrate a fistula.
Treatment and prognosis
Surgical resection of the fistula and abnormal segment of the bowel is usually required for a cure, although in the setting of malignancy, this suggests advanced disease (T4) making surgery complex.
In such cases, if palliation only is required then defunctioning colostomy, colonic stent placement or a nephrostomy may be required 3.




















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.