
Congenital lobar overinflation (CLO), also known as congenital lobar emphysema or congenital alveolar overdistension, is a congenital lung abnormality that describes overdistension of one or more pulmonary lobes.
On this page:
Epidemiology
Congenital lobar overinflation affects approximately 1: 25,000 live births and is more common in males (M: F = 3:1) 5,8.
Associations
Congenital lobar overinflation may be associated with an aberrant left pulmonary artery 7 and also with congenital heart defects:
Clinical presentation
Most cases present with respiratory distress within the first six months of life, about 30% at.birth and 50% within 1 month 5. Respiratory distress may be accompanied by wheezing and can develop rapidly or slowly; some cases may be unsuspected for years depending on the size of the abnormal lobe.
14% of cases have associated cardiac anomalies and anomalies of the kidney, gastrointestinal tract and skin have been reported
Pathology
CLO usually affects one lobe only:
the left upper lobe accounts for about 45% of cases
right middle lobe about 30%
right upper lobe 20%
lower lobes between 2 and 10% 6
Mass-like overdistension compresses the remaining lung and displaces the mediastinum
The condition is the end result of various disturbances of lung development and in 50% no cause is found. Airway obstruction is found in 25%. Associations include:
ball-valve obstruction of an airway
vascular anomalies compressing an airway
masses such as teratoma or foregut cyst
bronchial atresia is sometimes associated.
Histology may show enlarged distal airways and airspaces together or normal conducting airways with dilated and abnormally numerous alveoli. Sometimes the bronchial cartilage is abnormal or there are abnormal mucosal folds or granulation tissue which might cause obstruction. There is no emphysema.
Radiographic features
Radiograph
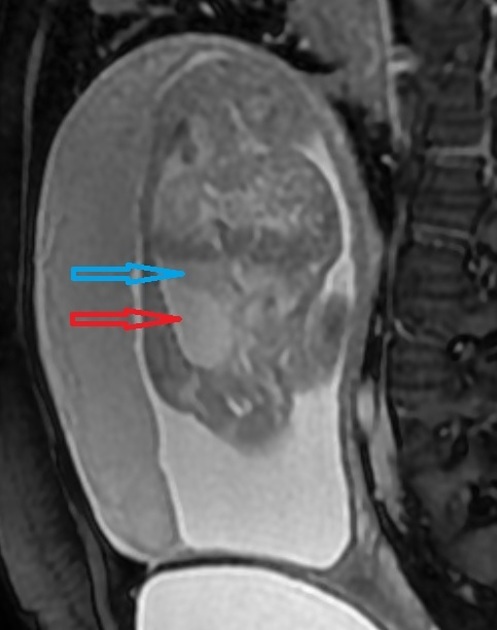
Immediate postpartum period
The affected lobe tends to appear opaque and homogeneous because of foetal lung fluid or it may show a diffuse reticular pattern that represents distended lymphatic channels filled with fetal lung fluid.
Later findings
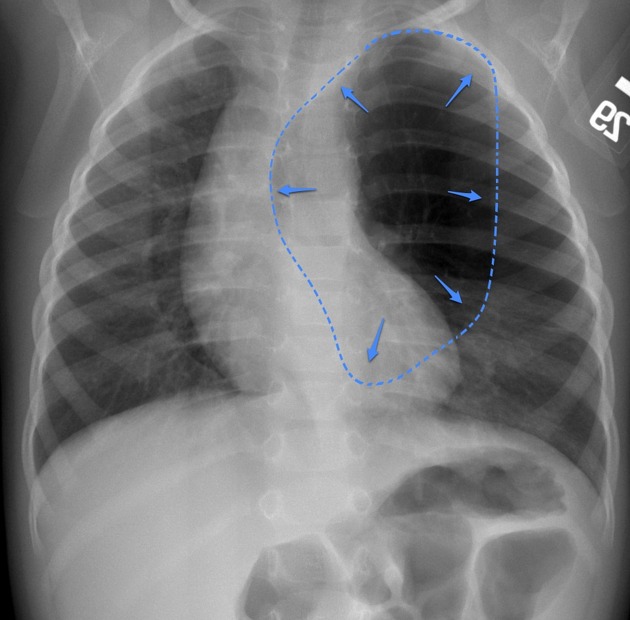
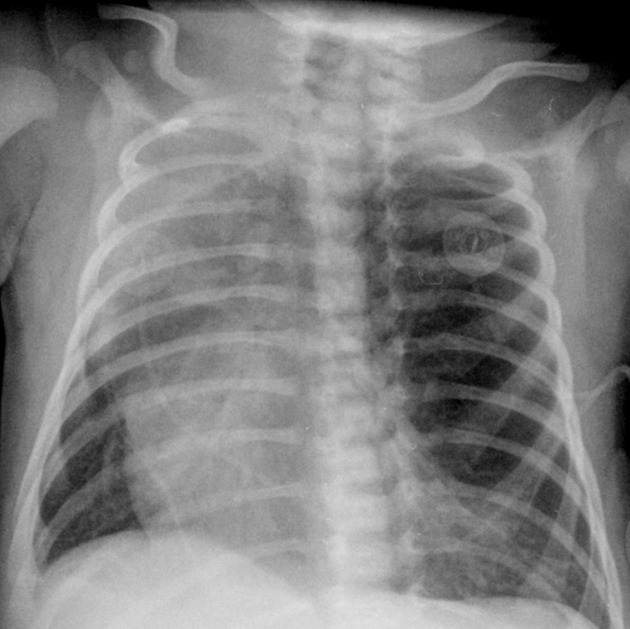
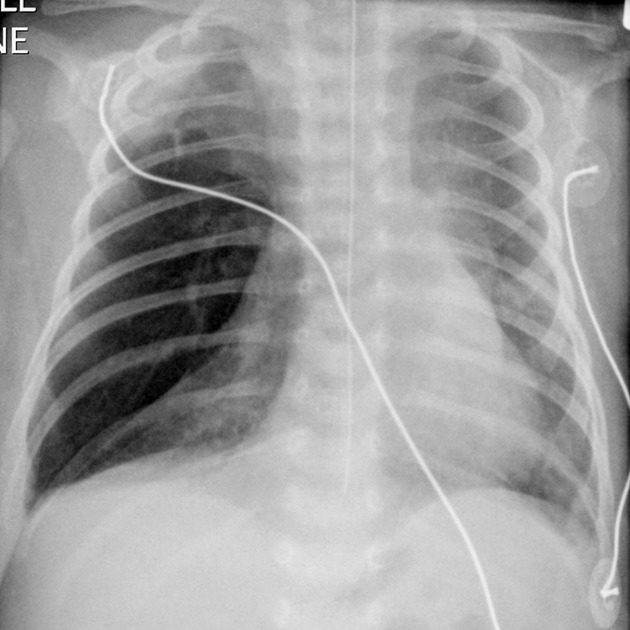
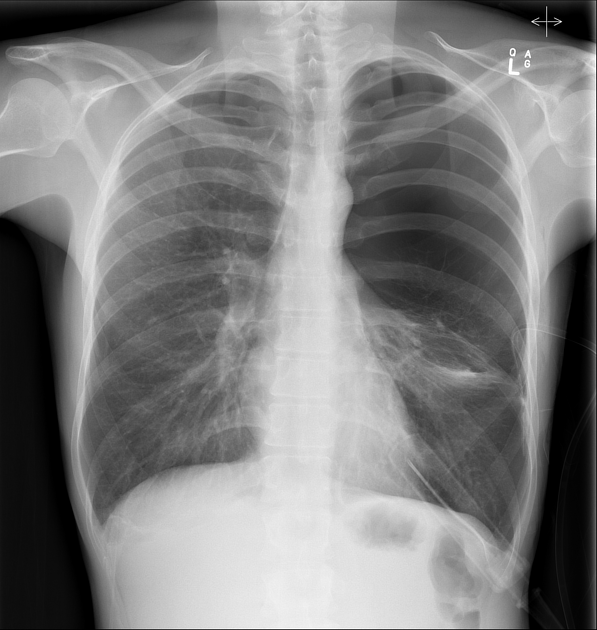
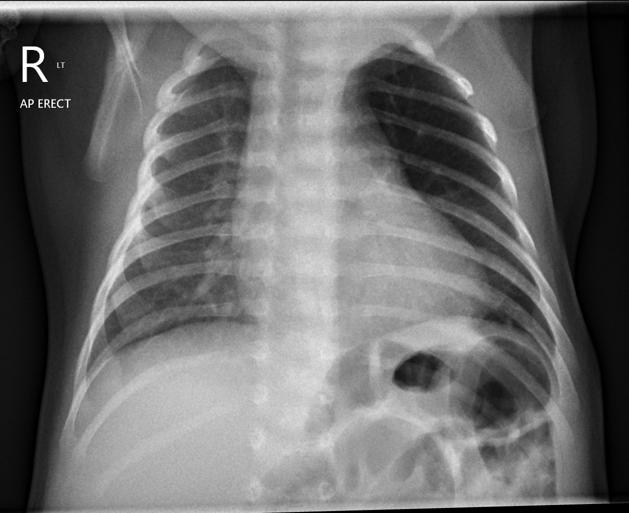
appears as an area of hypertransradiancy in the lung with oligemia
mass effect with mediastinal shift and hemidiaphragmatic depression
lateral decubitus film with the patient lying on the affected side will show little or no change in lobe volume
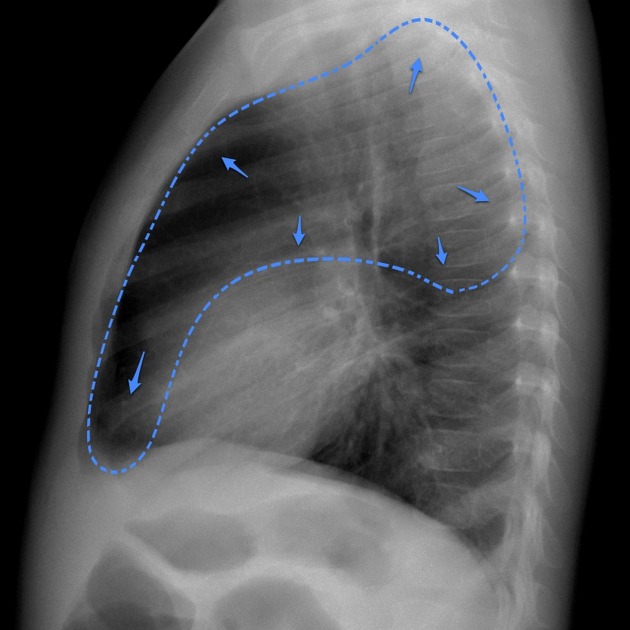
lateral film may show posterior displacement of the heart
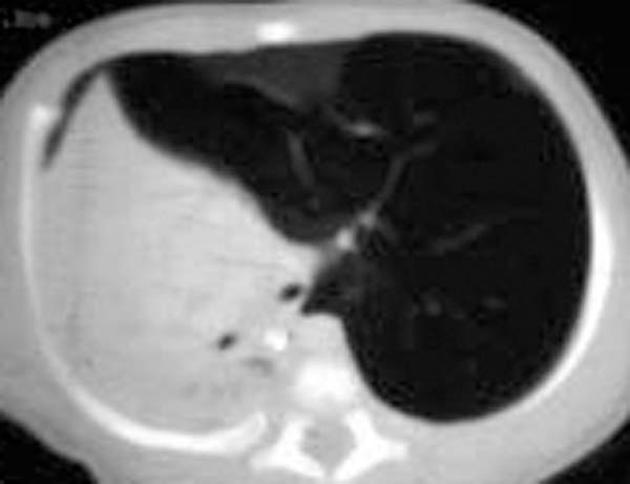
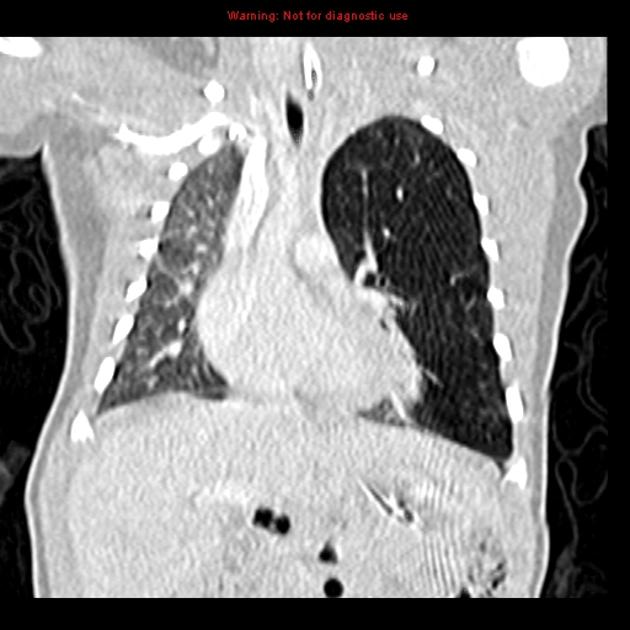
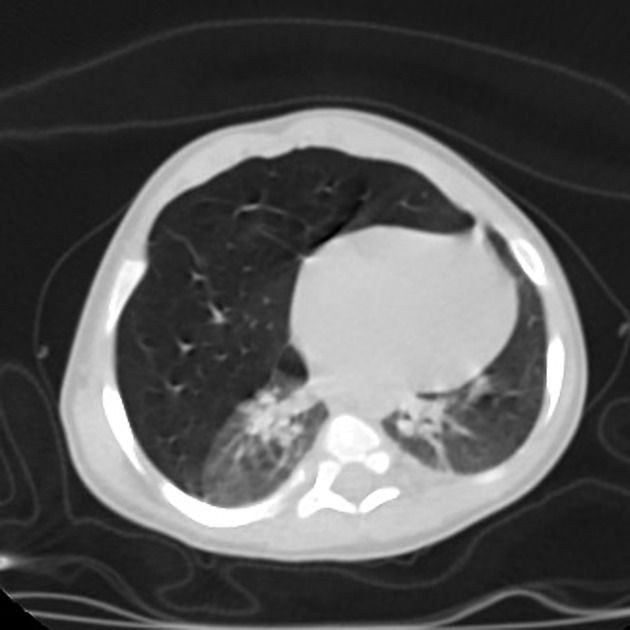
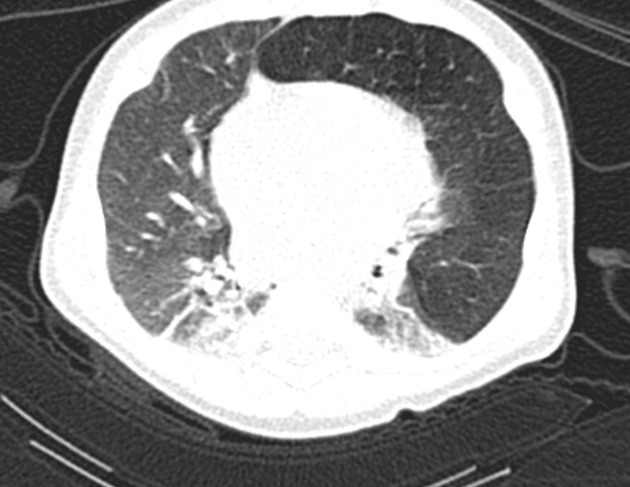
CT
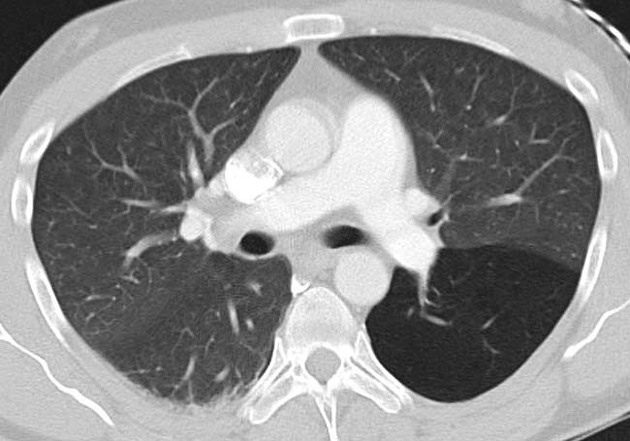
CT is usually performed to confirm the diagnosis, evaluate the mediastinal vascular structures, and to rule out other abnormalities. CT displays:
lobar hypertransradiancy
attenuated and sparse vessels in the affected lobe 4
may also show compressive atelectasis of adjacent lobes
mediastinal and diaphragmatic displacement
other congenital abnormalities
Treatment and prognosis
Mildly symptomatic patients are usually followed up. Surgical resection (lobectomy) is performed in severe cases 3.
Differential diagnosis
General imaging differential considerations include:
bronchial atresia: the parenchyma distal to the atretic segment can have air trapping
filamin A mutation
See also
differential for unilateral transradiant hemithorax









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.