
CSF rhinorrhea refers to a symptom of cerebrospinal fluid (CSF) leakage extracranially into the paranasal sinuses, thence into the nasal cavity, and exiting via the anterior nares. It can occur whenever there is an osseous and dural defect of the skull base that communicates directly or indirectly via paranasal or mastoid sinuses with the nasal cavity and nasopharynx.
On this page:
Clinical presentation
CSF rhinorrhea presents as intermittent, often positional, discharge of clear fluid from the nose.
Additionally, the communication between the normally sterile subarachnoid space and the nasal cavity allows pathogens entry, resulting in a lifetime risk of meningitis of 19% 10.
Diagnosis is usually confirmed biochemically by detecting beta-2-transferrin (asialotransferrin or tau-transferrin) or beta-trace protein in the fluid 8,10,14.
Pathology
Etiology
In the absence of trauma or surgery, idiopathic intracranial hypertension is a common and important etiology, particularly as surgical repair of these defects without treatment of the underlying cause has high recurrence rates 7.
Other etiologies include 4:
-
congenital
-
acquired
traumatic: closed head trauma with an anterior base of skull fracture is the most common cause of CSF rhinorrhea 2; natural barriers between the anterior cranial fossa and paranasal sinuses can be disrupted, leading to rhinorrhea, depending on the severity of trauma
-
iatrogenic
multiple neurosurgical procedures involving the skull base, e.g. transsphenoidal pituitary surgeries
complex operations at the skull base
otolaryngology procedures such as septoplasty and endoscopic surgery
-
non-traumatic
spontaneous: idiopathic intracranial hypertension with medial sphenoid meningocele formation
tumors: malignant nasopharyngeal and skull base tumors invading or involving the skull base can cause CSF rhinorrhea
Anatomical locations
CSF rhinorrhea can occur anywhere along the base of skull that communicates either directly or indirectly, via paranasal or mastoid sinuses, with the nasal cavity and nasopharynx.
Common sites include 4:
cribriform plate: it is the most common site for spontaneous CSF rhinorrhea
sphenoid: occur at the perisellar region and the lateral recess of the sphenoid sinus, especially in the setting of idiopathic intracranial hypertension
temporal bone and middle ear: common sites are the tegmen tympani and tegmen mastoideum
Radiographic features
CT
High-resolution bone CT
A high resolution non-contrast CT with thin bony algorithm reconstructions in multiple planes is an essential first step in diagnostic work up of a patient with suspected CSF rhinorrhea as it enable the identification of the location of a leak in a high proportion of cases (sensitivity 88-95%) by observing the ossous defect 10. Furthermore it fascilitates planning for surgical repair.
If multiple bony defects are detected, then additional imaging is required to confirm which is responsible for the leak.
CT cisternography
CT cisternography is useful in diagnosing an occult site of CSF leak or in determining which of multiple bony defects is responsible for the leak 4,8,10. It is performed after injecting contrast into the theca usually via a lumbar puncture and allowing it to mix throughout the CSF. This procedure is highly dependent on patient positioning and timing and requires a leak to be actively occurring during the study 10.
A leak can be confirmed by observing a streak of contrast or pooling of contrast in the anterior nasal cavity, paranasal sinus cavity and/or nasopharynx.
MRI
MRI has excellent contrast resolution without the disadvantage of ionizing radiation, however, it lacks the essential bony detail that CT can offer. As such it is usually only performed in addition to HRCT of the base of skull 10.
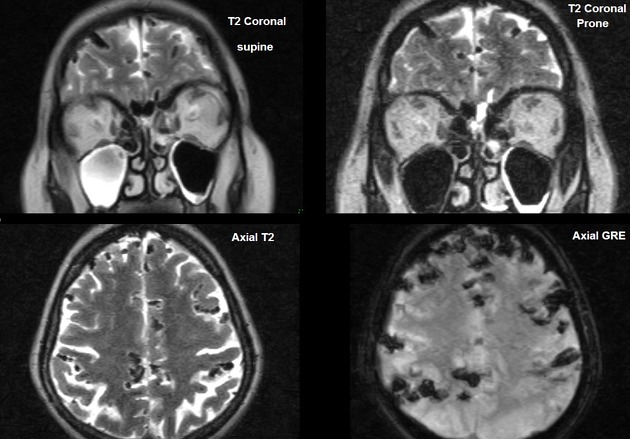
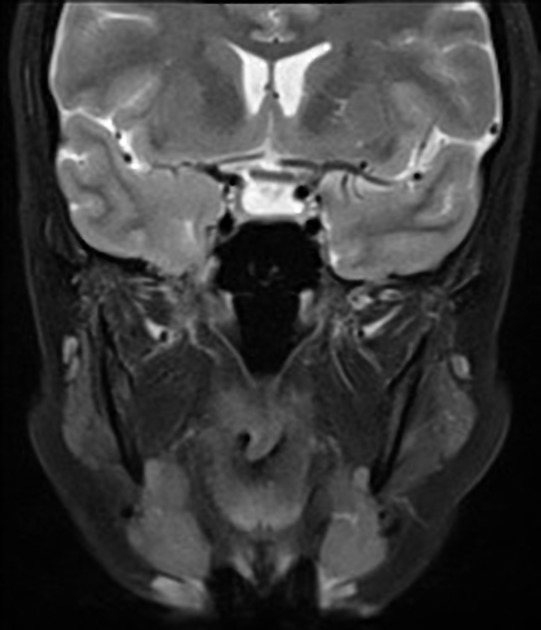
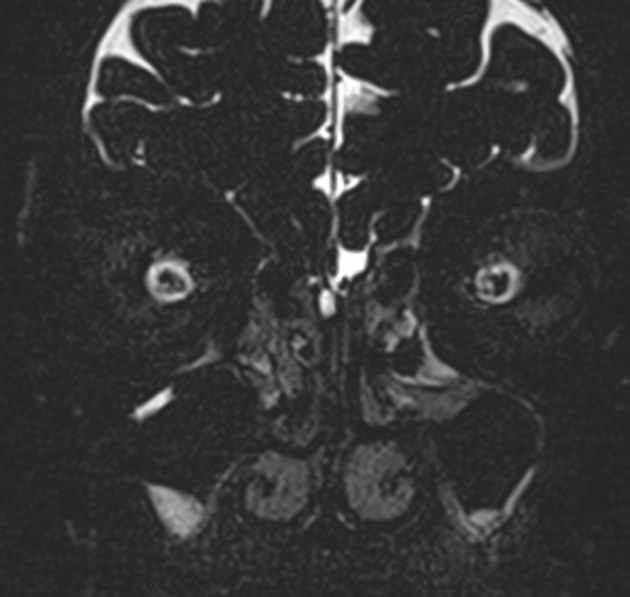
Heavily T2 weighted fat-saturated, preferably 3D, high-resolution sequences are capable of demonstrating a communication between the nasal cavity or paranasal sinuses and the subarachnoid space 10.
MR cisternography
MR cisternography is similar to CT cisternography, using a small amount of intrathecal gadolinium and allowing it to diffuse throughout the CSF. High resolution 3D fat saturated T1 weighted sequences can then identify high signal intensity CSF pooling within the nasal cavity or paranasal sinuses.
Proponents of the technique cite increased sensitivity compared to CT cisternography, without ionizing radiation 10.
Off-label warning: The use of gadolinium-based contrast agents for intrathecal administration is not approved by regulatory agencies such as the FDA. Read more: intrathecal gadolinium
Nuclear medicine
Radionuclide cisternography is reserved as a problem solving investigation in cases where a leak has not been identified using HRCT and citernography. A radiotracer (technetium-99 DTPA or indium-111 DTPA) is injected into the theca and pletgets are placed in both sides of the nasal cavity and radioactivity is then measured in each to determine if they have absorbed radiotracer-contating CSF 10.
Although potentially sensitive in diagnosing the presence of a leaks, as they will detect intermittent low-flow leaks, planar images and SPECT have poor anatomic resolution.
Cu-64 DOTA has been described as a PET-CT radiotracer 12.
Treatment and prognosis
Although historically craniotomy was performed for repair of the anterior cranial fossa leaks, endoscopic transnasal repair has become the mainstay of treatment 13.
History and etymology
Leakage of spinal fluid into either the nose or the ear was first described as a pathologic entity in 1899 by Sir St Clair Thomson (1859-1943), English laryngologist 3,9.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.