
Epidermal inclusion cysts or epidermal cysts are common cutaneous lesions that represent proliferation of squamous epithelium within a confined space in the dermis or subdermis.
On this page:
Terminology
These are occasionally termed sebaceous cysts, although this is a misnomer as the lesion does not originate in the sebaceous glands. As such, the term epidermal inclusion cyst is preferred.
These are also called epidermoid cysts, which in turn are sometimes considered a type of dermoid cyst 9.
Clinical presentation
Epidermal cysts are either found incidentally or present as a firm non-tender lump. If they rupture a local inflammatory response to the necrotic debris released can mimic infection. Although they can be found anywhere, they are typically located on the scalp, face, neck, trunk, and back 1. Rarely they can be seen within bones representing an intraosseous epidermoid cyst 2.
Rarely epidermal cysts can undergo malignant degeneration with squamous cell carcinoma 1.
Pathology
They are thought to occur as a result of 1,2:
traumatic/surgical implantation
occlusion of the pilosebaceous unit
congenital rests of cells
human papillomavirus type 57 or 60 infections implicated palmoplantar epidermoid cysts 1
They are closely related to cholesteatomas, and should not be confused with epidermoid cysts of the CNS.
Radiographic features
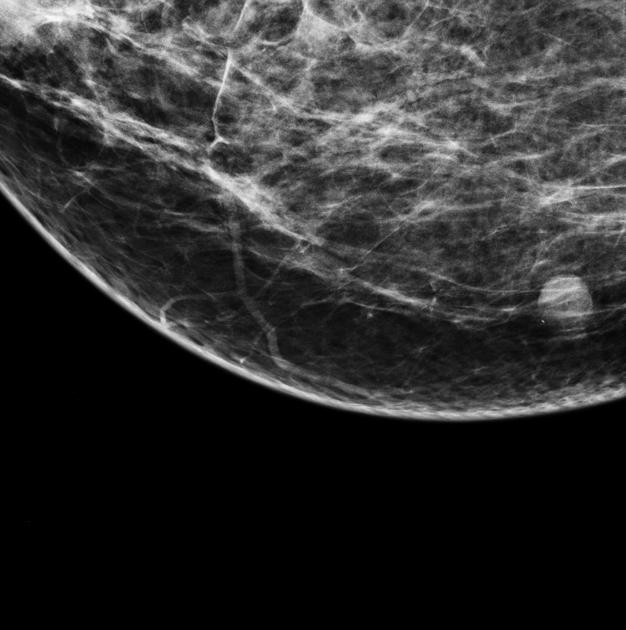
On all modalities, they appear as well-circumscribed masses arising in or just deep to the skin.
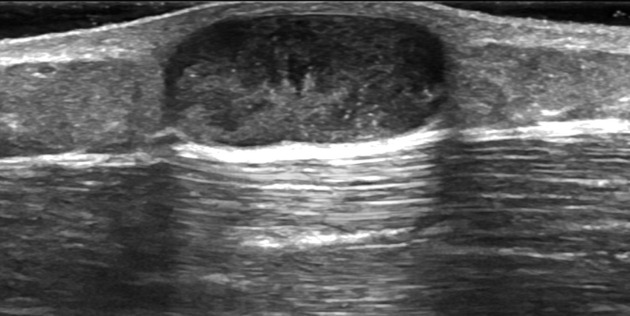
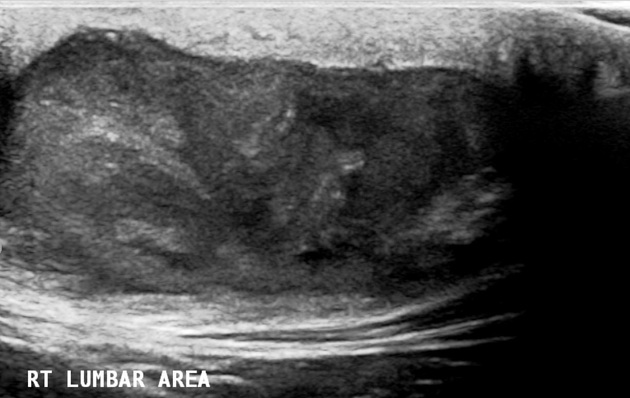
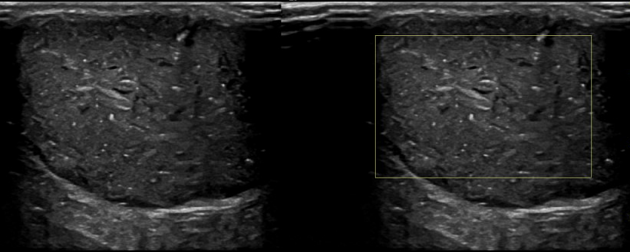
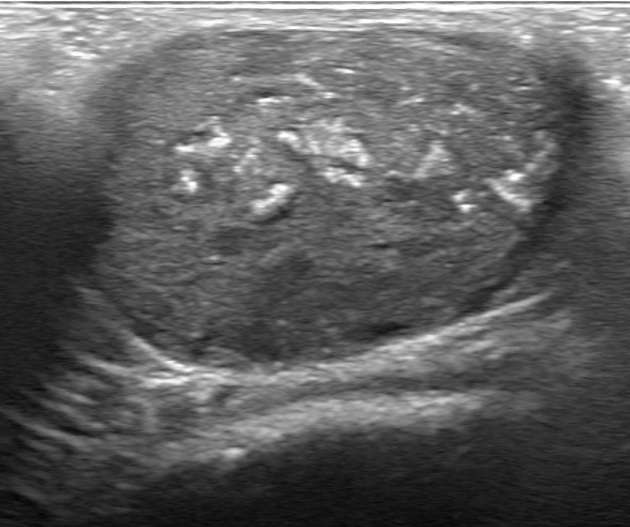
Ultrasound
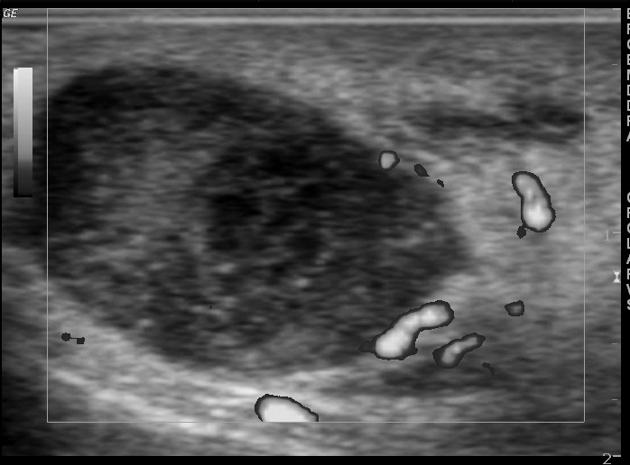
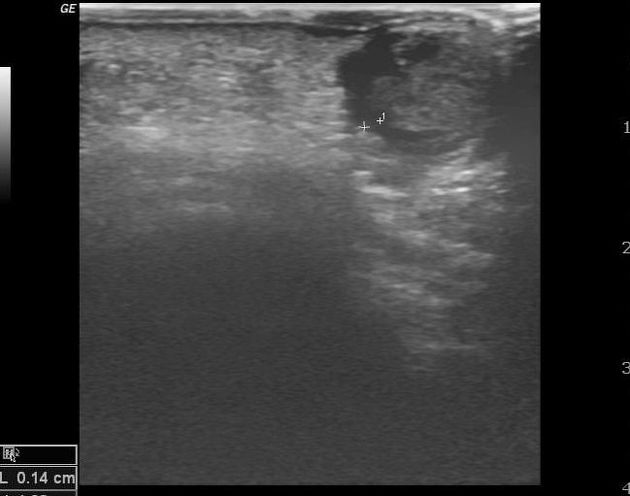
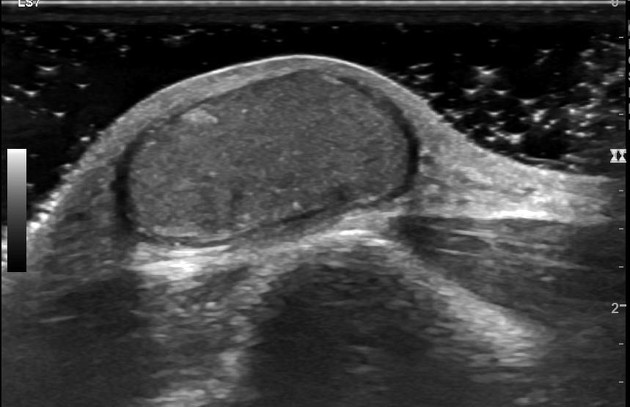
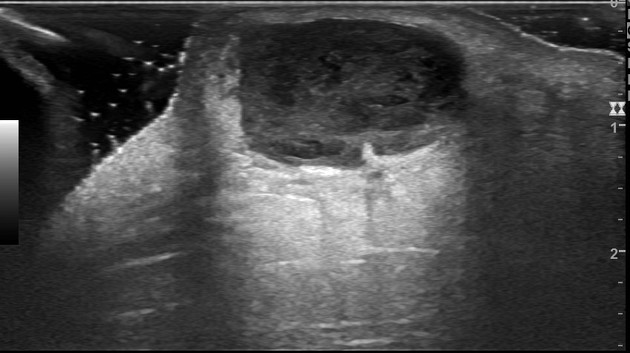
Well-circumscribed predominantly hypoechoic mass. Typical shapes include 6:
ovoid to spherical: ~70%
lobulated: ~20%
tubular: ~8%.
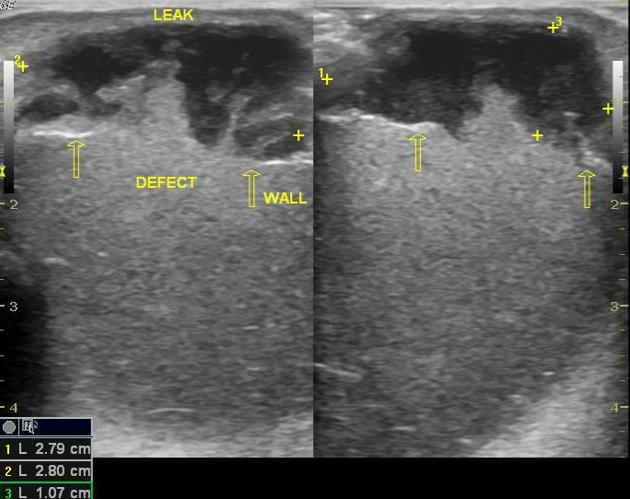
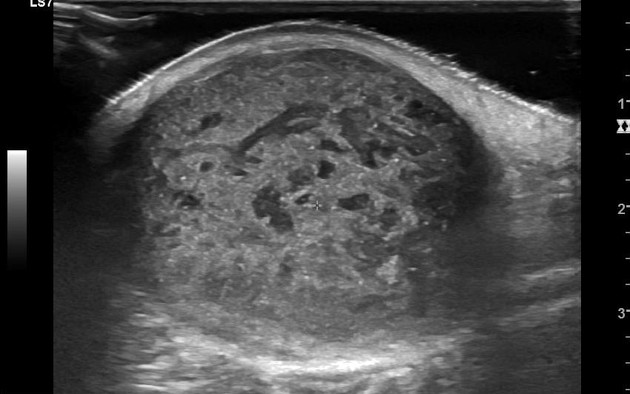
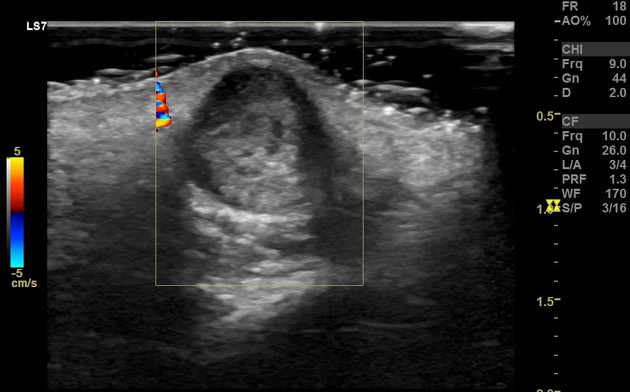
If small, it can mimic a typical anechoic cyst. Using subcutaneous fat as a reference, lesions tend to be hypoechoic. Larger lesions can be a little heterogeneous due to the presence of mucoid material, fat, calcification or pus. There is usually no associated vascularity. They can have a variable appearance when ruptured, occasionally associated with vascularity and lobulated contours 6. On color Doppler, it may show twinkling artifact 8.
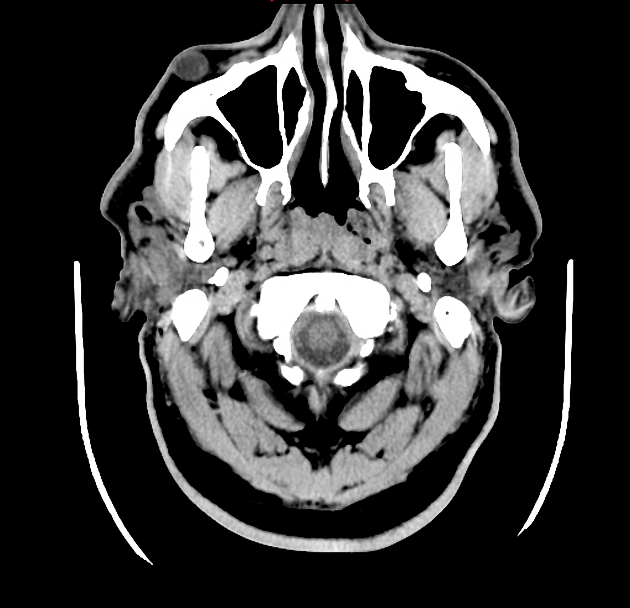
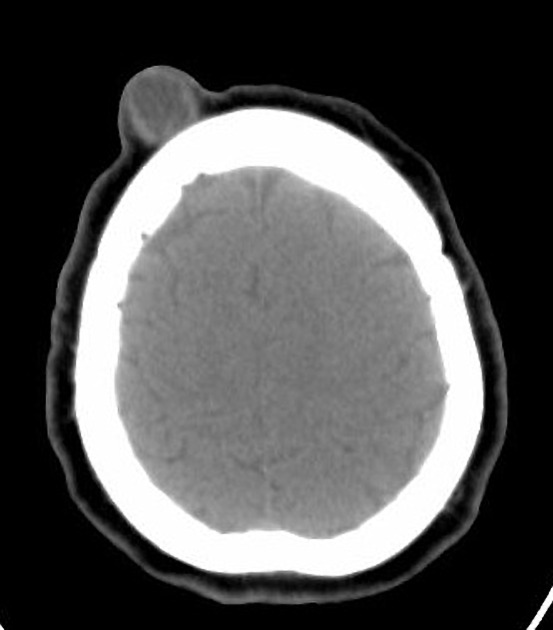
CT
The density of epidermal inclusion cysts is similar to that of water. The margins are usually thin and sclerotic.
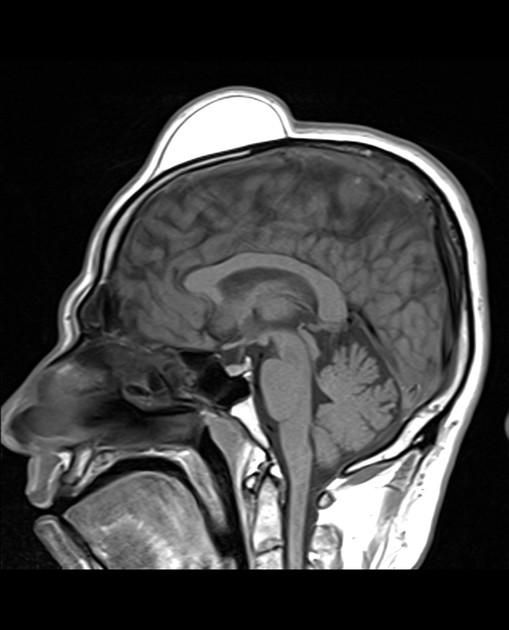
MRI
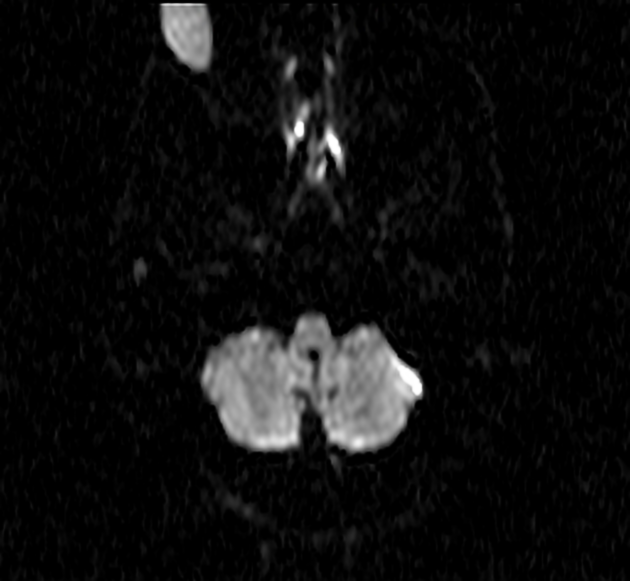
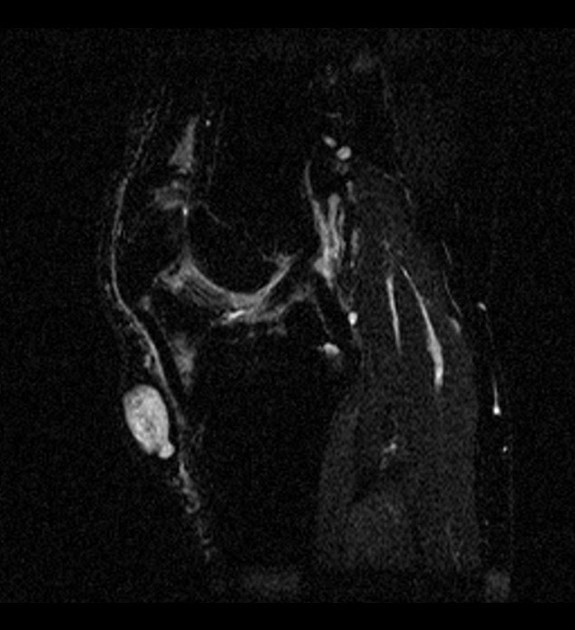
Imaging on MRI is similar to that of CNS epidermoid cysts or cholesteatomas, namely the content of the cyst is similar to water. In unruptured cases, the typical signal characteristics are:
T1: low/intermediate signal
T2: high signal
-
DWI
some true restricted diffusion (similar to soft tissue on ADC)
superimposed T2 shine through
-
T1 C+ (Gd)
no enhancement centrally
may have thin peripheral enhancement
Ruptured cysts may have septa, thick and irregular rim enhancement and can be accompanied by fuzzy enhancement in surrounding subcutaneous tissues 1.
Treatment and prognosis
They are benign and generally do not require treatment. If infected they may require incision and drainage. If they continue to grow they may require excision.
Complications
superimposed infection
rupture
concurrent occurrence of tumors within them, e.g. melanoma (very rare) 4
Differential diagnosis
General imaging differential considerations include:
ganglion cyst (if near a joint)














 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.