
The Fontan procedure is a repair surgical strategy for congenital cardiac anomalies. It is not usually used in isolation, but in combination with other repair procedures in a staged manner in an attempt to correct the underlying cardiac pathology.
On this page:
Rationale
The procedure attempts to bypass the right heart. Systemic circulation is redirected into the pulmonary arteries.
It can be used in multiple situations, including:
- tricuspid atresia
- hypoplastic left heart (part of the overall repair strategy)
- hypoplastic right heart
- other types of single ventricle physiology
Procedure
The original procedure involved:
- closure of atrial septal defect (ASD) and tricuspid valve
- creation of an anastomosis between the right atrial appendage and the main pulmonary artery
Modified Fontan procedure
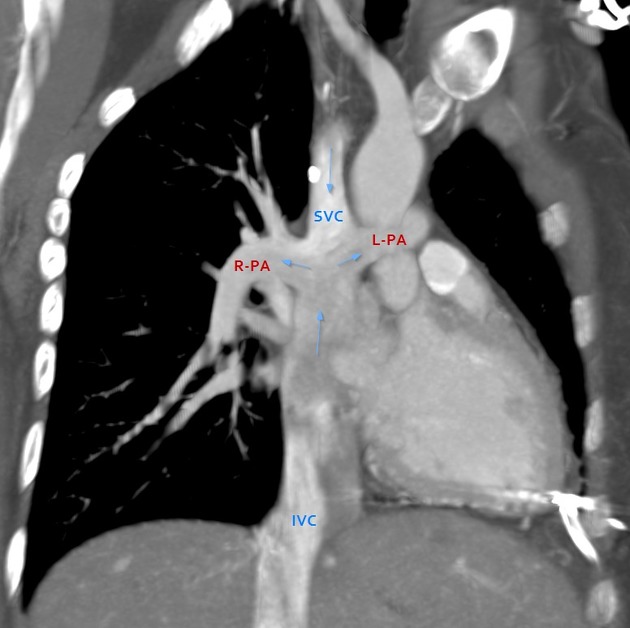
In order to improve flow dynamics, the original procedure has been modified and approaches developed which provide superior flow to the pulmonary circulation. The modified procedures involve creating a total cavopulmonary anastomosis, such that systemic venous return from both superior (SVC) and inferior vena cava (IVC) both supply the pulmonary arterial system.
There are two primary approaches: the "lateral tunnel" versus the "extracardiac conduit". In both situations, the SVC is divided at the superior cavoatrial junction and connected to the right pulmonary artery (i.e. bidirectional Glenn shunt). The difference is in the technique used to route IVC blood to the pulmonary artery:
-
lateral tunnel 7, 8
- a patent connection at the superior cavoatrial junction is established between the right atrium and the inferior aspect of the right pulmonary artery
- through an atriotomy, a synthetic or pericardial baffle is placed, which effectively bisects the right atrium, creating a passageway laterally for caval blood to reach the right pulmonary artery while leaving a more "normal" neo-atrium medially
- a sharp instrument is frequently used to create a 4-5 mm fenestration in the baffle, in order to allow some degree of pulmonary-to-systemic (right-to-left) shunting
-
extracardiac conduit
- no atrial-pulmonary connection is established
- IVC is divided at the inferior cavoatrial junction, and the defect at the inferior right atrium is closed
- a synthetic conduit is used to connect the transected IVC to the inferior aspect of the right pulmonary artery. The conduit courses adjacent to the right atrium
- a small connection between the conduit and the right atrium may be created, serving the same purpose as a fenestration (right-to-left shunt)
The intent of both of these procedures is to provide superior systemic-to-pulmonary flow while maintaining as much normal right atrium as possible in order to avoid arrhythmia.
The merits of each approach remain under study. In general, the extracardiac conduit results in less manipulation of the right atrium but is prone to conduit complications.
Treatment and prognosis
Although a palliative procedure, patients treated with the Fontan procedure can reach adulthood. The maximum duration of the procedure is not well-defined.
A patient with a failing Fontan repair can receive an extracardiac Fontan conduit if they do not already have one. The definitive procedure is cardiac transplantation.
Intracardiac and central venous thromboses are major causes of morbidity and mortality in patients after the Fontan procedure. This can occur in 1%-33% 4. Patients with a fenestrated baffle or conduit are frequently maintained on pharmacologic anticoagulation in order to reduce the risk of stroke from paradoxical emboli 8.
History and etymology
The procedure was originally suggested in 1971 by F Fontan and E Baudet as a correction for tricuspid atresia.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.