
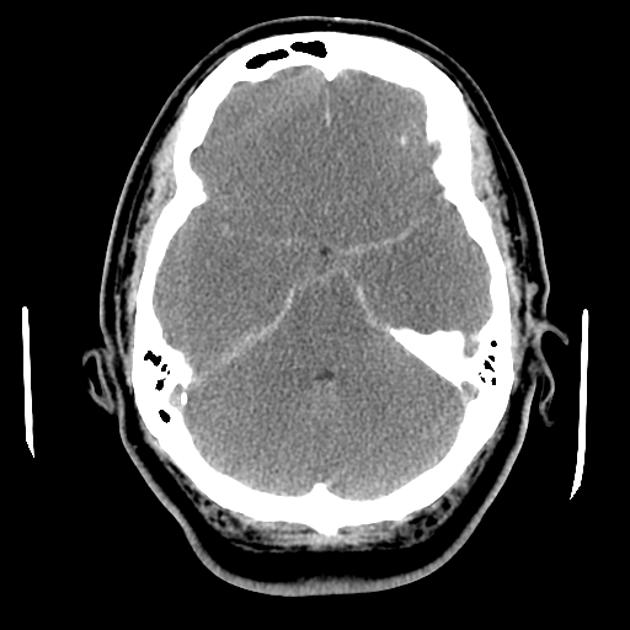
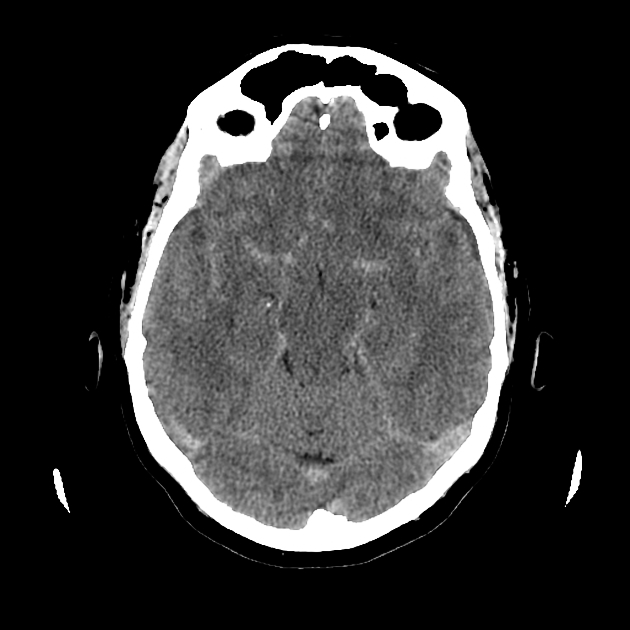
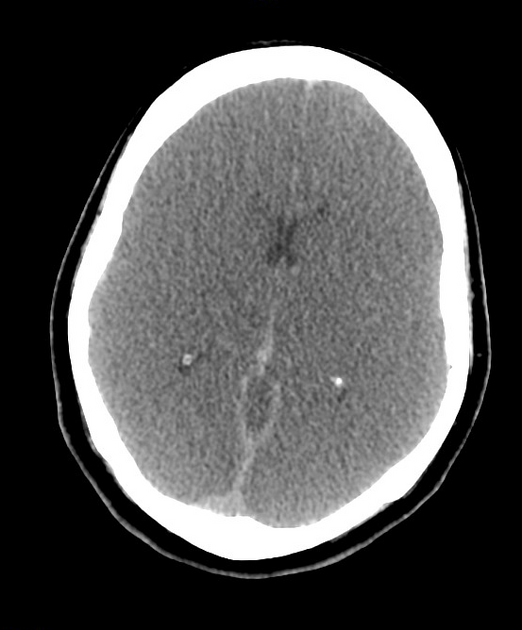
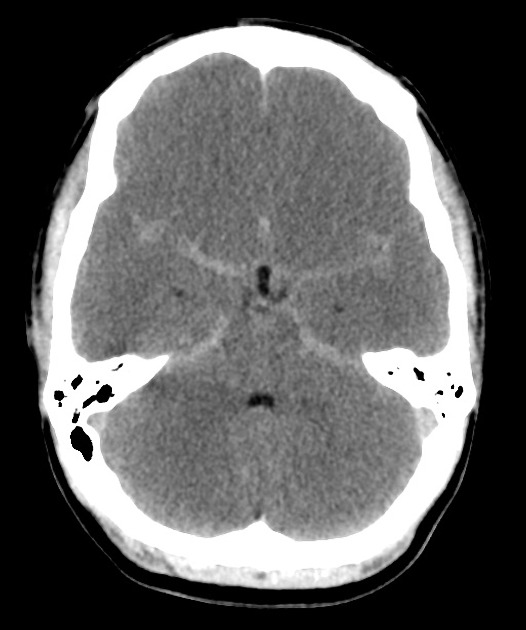
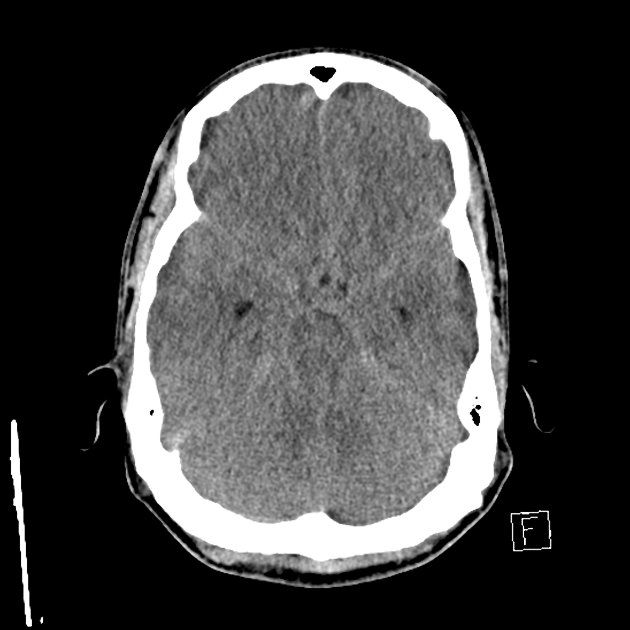
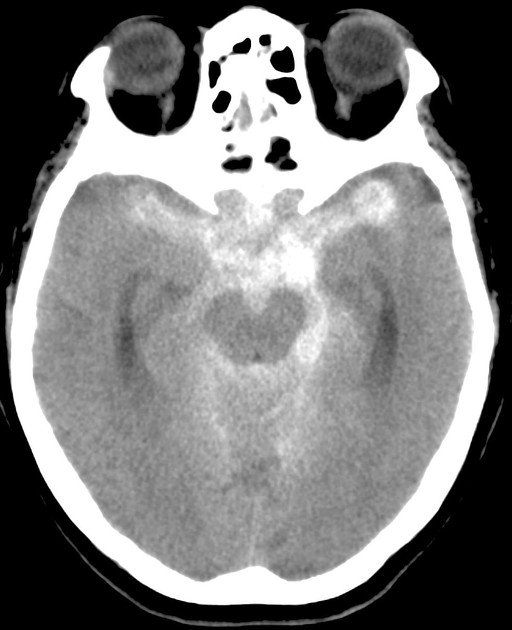
Pseudosubarachnoid hemorrhage describes an apparent increased attenuation within the basal cisterns simulating true subarachnoid hemorrhage. It is usually due to cerebral edema.
On this page:
Pathology
Etiology
The most common cause is cerebral edema where there is a decrease in parenchymal attenuation and engorgement and dilatation of the superficial venous structures due to an increased intracranial pressure 1,2. This typically occurs in the setting of hypoxic-ischemic brain injury (e.g. after recent resuscitation from cardiopulmonary arrest).
Other causes of pseudosubarachnoid hemorrhage include:
severe meningitis: breakdown of the blood-brain barrier allowing mildly hyperdense proteinaceous material to leak into the subarachnoid space 3
bilateral large subdural hemorrhage producing effacement of sulci and basal cisterns and the false impression of blood in the subarachnoid space 5
severe hyponatremia 6
intrathecal contrast
Radiographic features
CT
usually, symmetrical density confined to the basal cisterns (i.e. no sulcal density)
30-40 HU (cf. true acute subarachnoid hemorrhage ~60 HU)
often seen with generalized cerebral edema or basal cistern effacement
-
the appearances are thought to be due to a combination of
cisternal effacement
distention +/- thrombosis of vessels
adjacent brain hypoattenuation accentuating contrast difference
Given et al. reviewed 7 cases of generalized cerebral edema accompanied by increased basal cisternal attenuation which were all found not to have subarachnoid blood at lumbar puncture or autopsy 1.
Differential diagnosis
acute meningitis mimicking a subarachnoid hemorrhage 3






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.