
Stanford classification of aortic dissection
Updates to Article Attributes
Along with the DeBakey classification, the Stanford classification is used to separate aortic dissections into those that need surgical repair, and those that usually require only medical management. The Stanford classification divides dissections by the most proximal involvement:
-
type A: A affects ascending aorta and arch
- accounts for ~60% of aortic dissections
- surgical management
- may result in:
- coronary artery occlusion
- aortic incompetence
- rupture into the pericardial sac with resulting cardiac tamponade
-
type B: B begins beyond brachiocephalic vessels
- accounts for ~40% of aortic dissections
- dissection commences distal to the left subclavian artery
- medical management with blood pressure control
In 2014, a special report was published in Radiology 4 that recognised an uncommon form of aortic dissection. The authors describe dissections that originate from the arch or extendsextend proximally into the arch without the involvement of the ascending aorta which isare not adequately accounted for in the Stanford nor the DeBakey classification systems. Dissections in this region and, without the involvement of the ascending aorta proximal to the brachiocephalic trunk, are managed medically rather than surgically, provided there is no end-organ ischaemia. Hence, the authors proposed that any dissection originating from the arch between the brachiocephalic trunk and left subclavian artery and not involving the ascending aorta proximal to the brachiocephalic trunk be classified as a type B dissection. See case 10 for an example.
-<li>rupture into pericardial sac with resulting <a href="/articles/cardiac-tamponade">cardiac tamponade</a>- +<li>rupture into the pericardial sac with resulting <a href="/articles/cardiac-tamponade">cardiac tamponade</a>
-</ul><p>In 2014, a special report was published in <a title="Radiology (journal)" href="/articles/radiology-journal">Radiology</a><sup> 4</sup> that recognised an uncommon form of aortic dissection. The authors describe dissections that originate from the arch or extends proximally into the arch without the involvement of the ascending aorta which is not adequately accounted for in the Stanford nor the DeBakey classification systems. Dissections in this region and without the involvement of the ascending aorta proximal to the brachiocephalic trunk are managed medically rather than surgically, provided there is no end-organ ischaemia. Hence, the authors proposed any dissection originating from the arch between the brachiocephalic trunk and left subclavian artery and not involving the ascending aorta proximal to the brachiocephalic trunk be classified as a type B dissection.</p>- +</ul><p>In 2014, a special report was published in <a href="/articles/radiology-journal">Radiology</a><sup> 4</sup> that recognised an uncommon form of aortic dissection. The authors describe dissections that originate from the arch or extend proximally into the arch without the involvement of the ascending aorta which are not adequately accounted for in the Stanford nor the DeBakey classification systems. Dissections in this region, without the involvement of the ascending aorta proximal to the brachiocephalic trunk, are managed medically rather than surgically, provided there is no end-organ ischaemia. Hence, the authors proposed that any dissection originating from the arch between the brachiocephalic trunk and left subclavian artery and not involving the ascending aorta proximal to the brachiocephalic trunk be classified as a type B dissection. See case 10 for an example.</p>
Image 2 Diagram (DeBakey III) ( update )
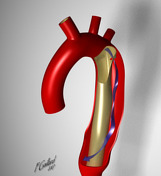
Image 3 CT (C+ arterial phase) ( update )

Image 5 CT (C+ arterial phase) ( update )

Image 6 CT (C+ arterial phase) ( update )

Image 7 CT (C+ arterial phase) ( update )

Image 8 CT (C+ arterial phase) ( update )

Image 9 CT (C+ arterial phase) ( update )

Image 10 CT (C+ arterial phase) ( update )

Image 11 CT (C+ arterial phase) ( create )

Image 12 CT (C+ arterial phase) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.