
Subependymal giant cell astrocytomas (SGCAs or alternatively SEGAs) are benign tumors (WHO grade 1), seen almost exclusively in young patients with tuberous sclerosis. They can be either asymptomatic or symptomatic due to obstructive hydrocephalus; surgical treatment is often curative.
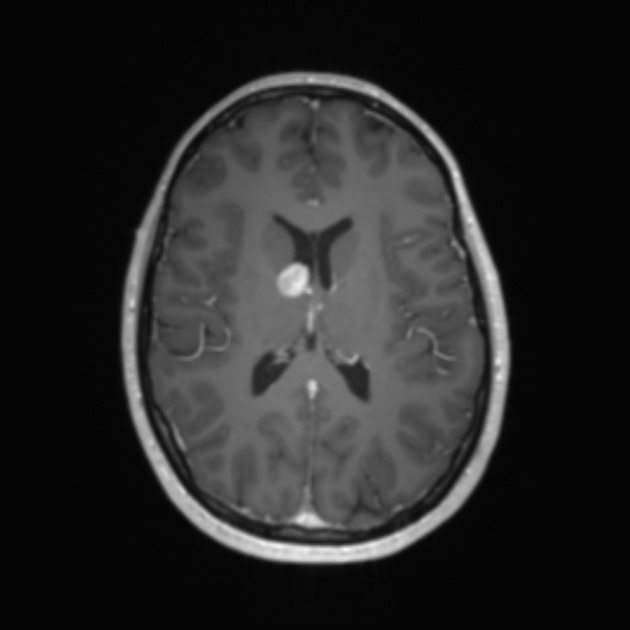
On imaging, they classically appear as an intraventricular mass near the foramen of Monro, larger than 1 cm, showing calcifications, heterogeneous MRI signal, and marked contrast enhancement.
On this page:
Epidemiology
Subependymal giant cell tumors are a well-known manifestation of tuberous sclerosis, affecting 5-15% of patients with the condition 8. They are principally diagnosed in patients under 20 years of age, only occasionally found in older individuals.
Although they are almost exclusively encountered in the setting of tuberous sclerosis, case reports of isolated subependymal giant cell astrocytomas in individuals with no other stigmata of tuberous sclerosis are available 9.
Clinical presentation
Subependymal giant cell tumors are often asymptomatic. When symptoms occur, they are usually a result of obstructive hydrocephalus because of the mass effect around the ventricular system at the level of the interventricular foramen (of Monro).
Pathology
Subependymal giant cell astrocytomas are designated circumscribed astrocytic gliomas and considered WHO grade 1 tumor in the 5th edition (2021) WHO classification of CNS tumors 10.
Due to their close association with tuberous sclerosis, they too are associated with mutation of TSC1 or TSC2 10.
Macroscopic appearance
These tumors are multilobulated well-circumscribed tumors arising from the wall of the lateral ventricles near the foramen of Monro. They frequently contain cysts and calcification 8.
Microscopic appearance
Subependymal giant cell astrocytomas are believed to arise from a subependymal nodule present in the ventricular wall in a patient with tuberous sclerosis, although this has yet to be categorically established 4,8.
Histologically, subependymal nodules and subependymal giant cell tumors are essentially indistinguishable, and the distinction lies in the potential for growth and mass effect 5. The cells that appear astrocytic, usually resemble gemistocytes (large polygonal cells with prominent eosinophilic cytoplasm) with a smaller number of ganglionic appearing giant pyramidal-like cells 8.
The ependymal lining over subependymal giant cell astrocytomas remains intact making CSF seeding highly unlikely 7.
Evidence suggests that they are of a mixed neuronal and glial lineage, although they continue to be classified as astrocytomas 5.
Immunophenotype
Immunohistochemical examination of these tumors demonstrates the following reactivity 8:
S100: positive
GFAP: variable
synaptophysin: variable
CD34: negative
additional variable and focal reactivity: class III beta-tubulin, NeuN, SOX2
Radiographic features
The foramen of Monro is the classic location, and the tumor arises when a subependymal nodule transforms into subependymal giant cell astrocytoma over a period of time.
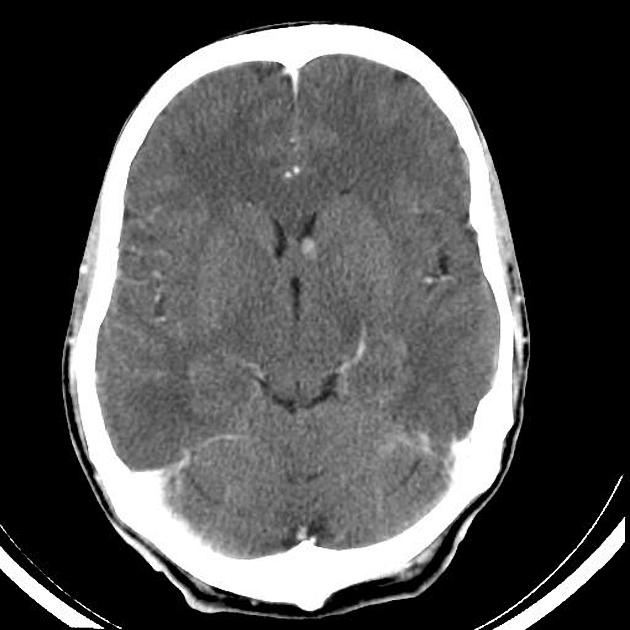
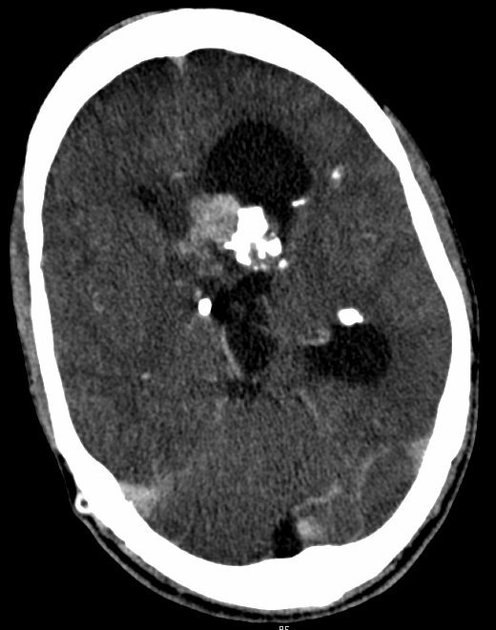
CT
intraventricular mass near the foramen of Monro
usually larger than 1 cm
iso- or slightly hypoattenuating to grey matter
calcification is common and hemorrhage is possible
accompanying hydrocephalus may be present
often shows marked contrast enhancement (subependymal nodules also enhance)
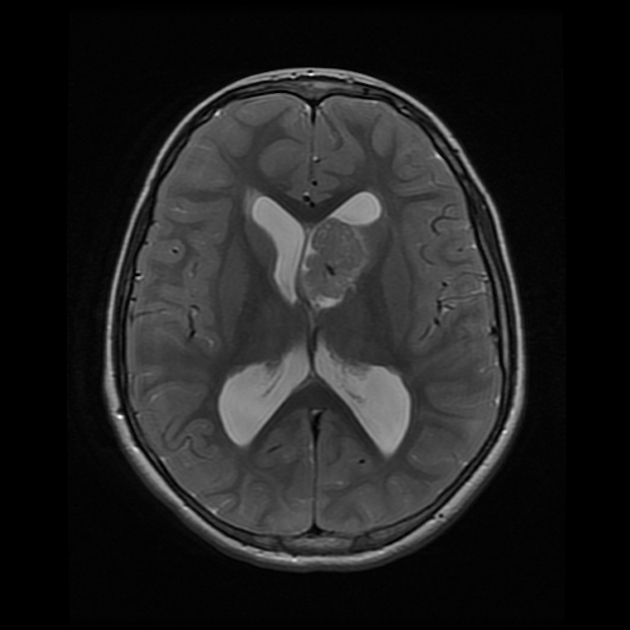
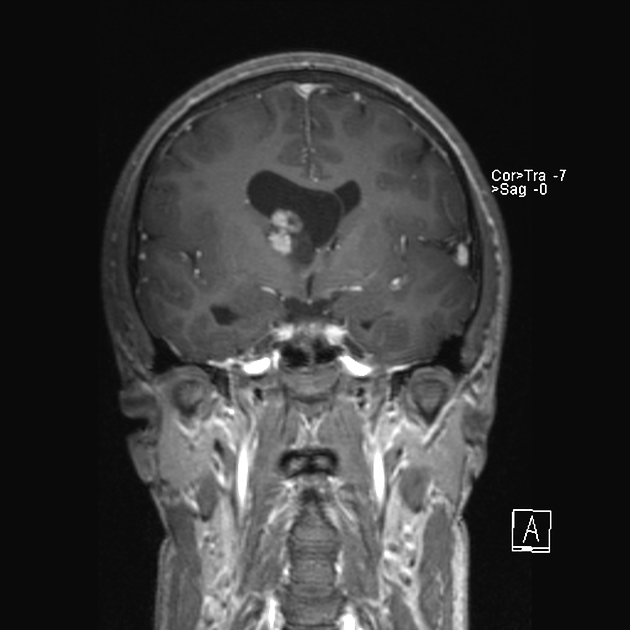
MRI
T1: heterogeneous and hypo- to isointense to grey matter
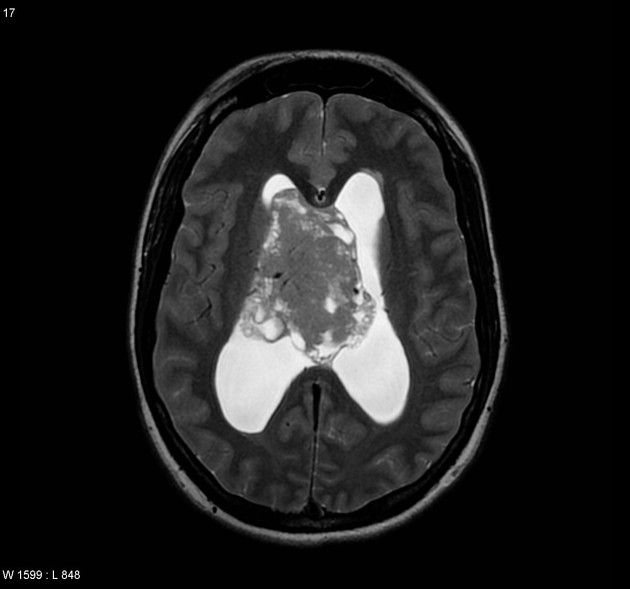
T2: heterogeneous and hyperintense to grey matter; calcified components can be hypointense
T1 C+ (Gd): can show marked enhancement
Treatment and prognosis
Young children who have tuberous sclerosis may be offered screening because of the increased risk of developing subependymal giant cell astrocytomas.
The main treatment is surgery, which is indicated if a tumor is symptomatic, or growth is demonstrated on MRI. Surgery is often curative. Oral mTOR inhibitors (e.g. everolimus or sirolimus) have also been trialed 3.
Differential diagnosis
In the clinical context of known tuberous sclerosis, the appearance is virtually pathognomonic, and the main differential is between a subependymal nodule and subependymal giant cell astrocytoma. Serial imaging is most helpful here, as growth implies the latter.
Other general considerations include:




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.