
Appendiceal mucoceles occur when obstruction of the appendiceal lumen causes mucus to accumulate and progressively distend the appendix. The term describes an imaging appearance rather than a pathological entity. The underlying causes lie on a spectrum between benign obstruction with retention cyst and malignant obstruction due to invasive mucinous adenocarcinoma.
On this page:
Epidemiology
The reported prevalence at appendectomy is 0.2-0.3%. They are thought to typically present in middle-aged individuals, particularly considering the epidemiology of the mucinous neoplasms. Though carcinoid tumor is the most common primary appendiceal neoplasm in surgical pathology series, mucoceles due to mucinous neoplasms are the most common appendiceal tumors detected on imaging 7.
Pathology
The term mucocele is simply a macroscopic description of an appendix that is grossly distended by mucus 7,12. They may be caused by either benign or malignant lesions, categorized by Peritoneal Surface Oncology Group International (PSOGI) in 2012 into the following types:
mucus retention cyst due to obstruction (most commonly by a fecolith or appendicolith)
serrated polyp (previously mucosal hyperplasia)
low-grade or high-grade appendiceal mucinous neoplasms (LAMN or HAMN): most common 11
Variants
myxoglobulosis: a rare mucocele variant seen with multiple small intraluminal globules which can calcify and produce 1-10 mm mobile calcifications
Radiographic features
Plain radiograph
It can be characterized by a right iliac fossa mass with peripheral calcifications 12.
Fluoroscopy
Barium enema
If a contrast examination is performed, there is usually non-filling or partial-filling of the appendix. Where there is a large mucocele, the associated mass effect can cause the indentation or lateral displacement of the cecum.
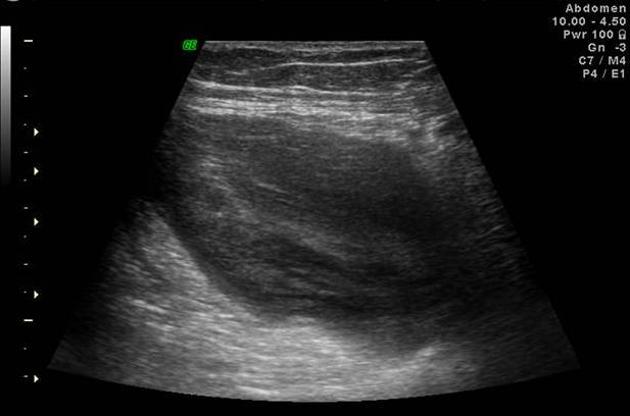
Ultrasound
Typically cystic mass with variable internal echogenicity 8. The presence of an "onion sign" (sonographic layering within a cystic mass) is considered a highly suggestive feature 2,6. Acoustic shadowing may be present due to the mural calcifications 12.
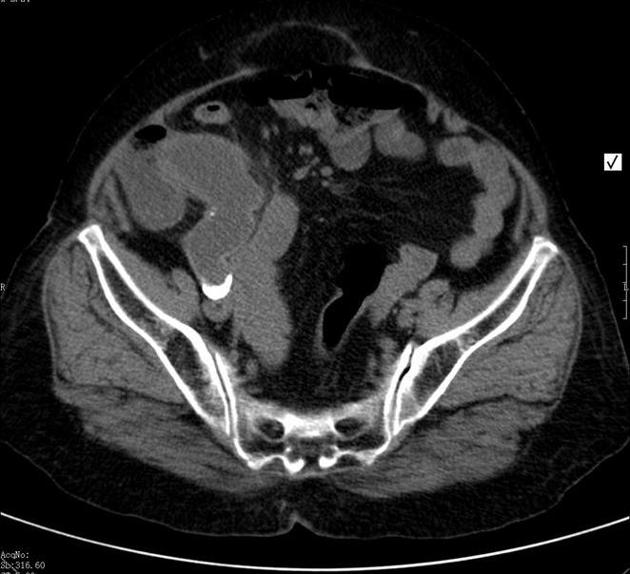
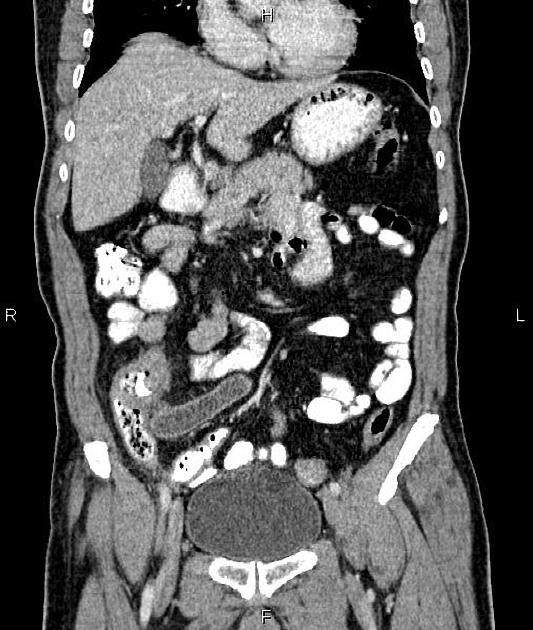
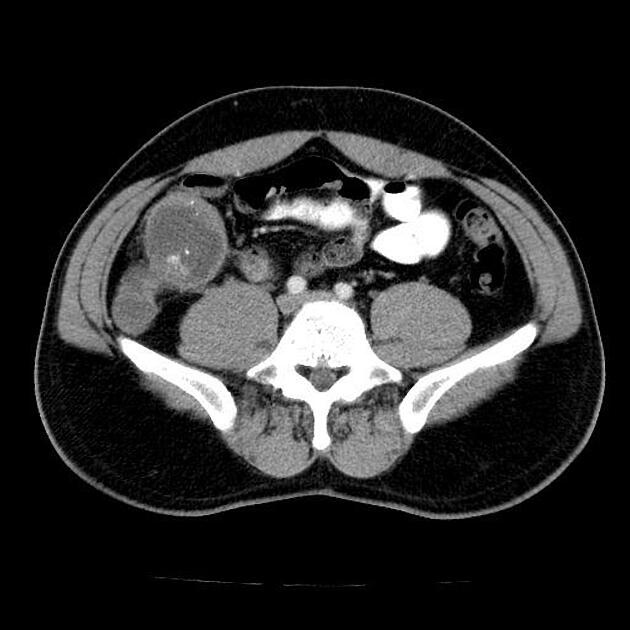
CT
They are typically seen as a well-circumscribed, low-attenuation, spherical, or tubular mass contiguous with the base of the cecum.
curvilinear mural calcification suggests the diagnosis but is seen in less than 50% of cases
intraluminal bubbles of gas or a gas-fluid level within a mucocele indicate the presence of superinfection, which can occur in both benign and malignant mucoceles
mural nodularity and irregular wall thickening are suggestive of a malignant process 12
When identifying a mucocele on CT, a search for extraluminal mucin is mandatory, which are low attenuation deposits commonly seen in certain locations 12:
periappendiceal space
peritoneal cavity
at the surface of abdominal viscera, including ovaries and bowel
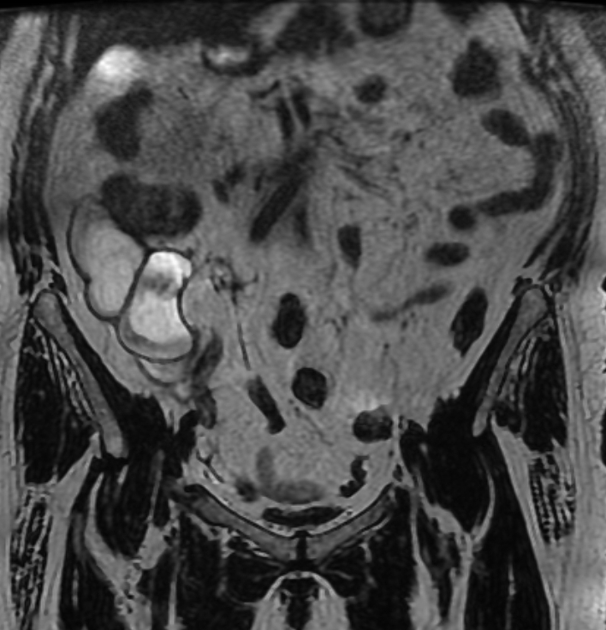
MRI
Seen as a rounded right iliac fossa mass and the typical signal characteristics include:
T1: depending on the mucin concentration, the signal may be variable, from hypointense to isointense 9
T2: hyperintense
Treatment and prognosis
Treatment is usually surgical.
Complications
rupture: may lead to pseudomyxoma peritonei (mucinous ascites) if the underlying cause is neoplastic 11,12
can act as a lead point and result in an ileocolic intussusception 9
History and etymology
In 1842, Rokitansky described appendiceal mucocele for the first time 15.
Differential diagnosis
Differentiating benign (non-neoplastic mucocele and mucinous cystadenoma) and malignant (mucinous cystadenocarcinoma) appendiceal lesions can be difficult on imaging. Wang et al. 10 found a statistically significant difference in wall irregularity and soft-tissue thickening between malignant and benign cases.
Appendicitis and appendiceal mucocele may be difficult to differentiate, and may sometimes coexist 12,13.
an outer diameter of 15 mm or more was predictive of mucocele of the appendix with a sensitivity of 83% and specificity of 92%13
cystic dilatation of the appendix, mural calcification, and a luminal diameter greater than 13-15 mm are considered features suggestive of coexisting mucocele in patients with acute appendicitis 13,14
Marotta et al. found that dilatation limited to the distal appendix in combination with mural calcification and diameter >2 cm are associated with malignancy 17



























 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.