
Bladder calculus
Updates to Article Attributes
Bladder calculi occur either from migrated renal calculi or urinary stasis. Bladder calculi can be divided into primary and secondary stones:
- primary: stones form de novo in the bladder
- secondary: stones are either from renal calculi which have migrated down into the bladder, or from concretions on foreign material (e.g. urinary catheters)
Epidemiology
Primary bladder calculi, in otherwise normal bladders, were previously common, but are now very uncommon in western nations 2. When encountered, the most common cause is due to urinary stasis, including from:
Family history is found in up to one third of idiopathic cases 2.
Clinical presentation
Bladder calculi may present with pain, infection, haematuria or may be asymptomatic.
Radiographic features
Plain Filmfilm
Usually densely radio-opaque, calculi may be single or multiple and often large. Frequently lamination is observed internally, like the skin of an onion.
Ultrasound
Sonographically they are mobile, echogenic, and shadow distally. They may be associated with bladder wall thickening due to inflammation.
Treatment and management
The earliest method of operative removal of bladder calculus was performed via the perineum with the patient in a supine position and the legs elevated - hence the term lithotomy position.
-</ul><p>Family history is found in up to one third of idiopathic cases <sup>2</sup>. </p><h4>Clinical presentation</h4><p>Bladder calculi may present with pain, infection, haematuria or may be asymptomatic. </p><h4>Radiographic features</h4><h5>Plain Film</h5><p>Usually densely radio-opaque, calculi may be single or multiple and often large. Frequently lamination is observed internally, like the skin of an onion.</p><h5>Ultrasound</h5><p>Sonographically they are mobile, echogenic, and shadow distally. They may be associated with bladder wall thickening due to inflammation.</p><h4>Treatment and management</h4><p>The earliest method of operative removal of bladder calculus was performed via the perineum with the patient in a supine position and the legs elevated - hence the term lithotomy position.</p>- +</ul><p>Family history is found in up to one third of idiopathic cases <sup>2</sup>. </p><h4>Clinical presentation</h4><p>Bladder calculi may present with pain, infection, haematuria or may be asymptomatic. </p><h4>Radiographic features</h4><h5>Plain film</h5><p>Usually densely radio-opaque, calculi may be single or multiple and often large. Frequently lamination is observed internally, like the skin of an onion.</p><h5>Ultrasound</h5><p>Sonographically they are mobile, echogenic, and shadow distally. They may be associated with bladder wall thickening due to inflammation.</p><h4>Treatment and management</h4><p>The earliest method of operative removal of bladder calculus was performed via the perineum with the patient in a supine position and the legs elevated - hence the term lithotomy position.</p>
Image ( update )
Image 2 X-ray (Frontal) ( update )

Image 6 X-ray (Frontal) ( update )

Image 8 CT (C+ portal venous phase) ( update )

Image 9 CT (bone window) ( update )

Image 10 Ultrasound ( update )

Image 11 X-ray (Frontal) ( update )

Image 12 CT (non-contrast) ( update )
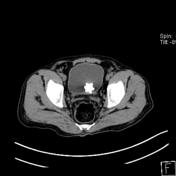
Image 13 X-ray (Frontal) ( update )

Image 14 X-ray (Frontal) ( update )

Image 15 CT (bone window) ( update )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.