
Gastroschisis refers to an extra-abdominal herniation (evisceration) of fetal or neonatal bowel loops (and occasionally portions of the stomach, liver, and/or bladder12) into the amniotic cavity through a para-umbilical anterior abdominal wall defect.
On this page:
Epidemiology
The estimated incidence is around 1-6 per 10,000 live births. There may be a male predilection and an increased incidence with younger maternal age.
Associations
Associated anomalies are rare with gastroschisis (unlike with an omphalocele) except for related bowel abnormalities (i.e. intestinal atresia, malrotation, or stenosis from vascular compromise).
A fetus with gastroschisis may have intrauterine growth restriction (IUGR) 6.
Pathology
This anomaly does not have a surrounding membrane (unlike an uncomplicated omphalocele). It is the small bowel that herniates most often. It always herniates through the abdominal wall defect and lacks normal rotation and fixation to the posterior abdominal wall.
In addition to the small intestine, the large intestine, stomach, portions of the genitourinary system and liver may herniate through the defect as well.
The defect is invariably on the right side and usually measures between 2-4 cm. There is no covering membrane or membrane remnant.
Etiology
A compromise in vascular supply to the area in the abdominal wall adjacent to the umbilicus may be a causative factor. Some also suggest an incomplete regression of the right umbilical vein as a possible causative factor.
Markers
maternal serum alpha-fetoprotein (MSAFP) may be elevated: the extent of AFP rise is often greater for gastroschisis than for an omphalocele
Genetics
Most cases have a sporadic occurrence.
Radiographic features
Ultrasound
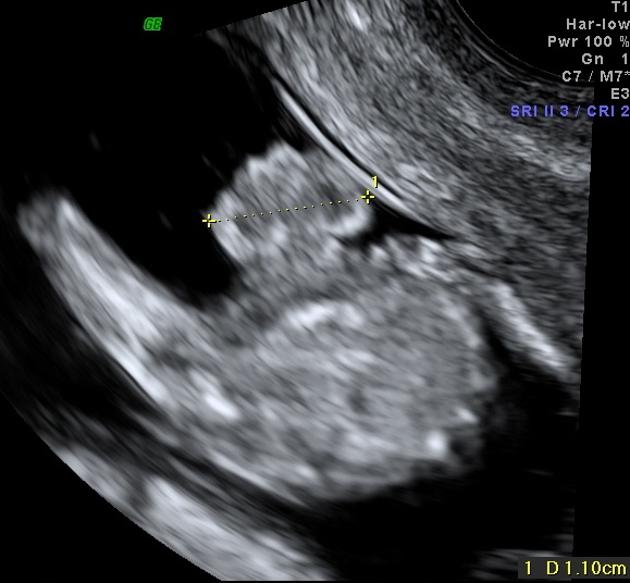
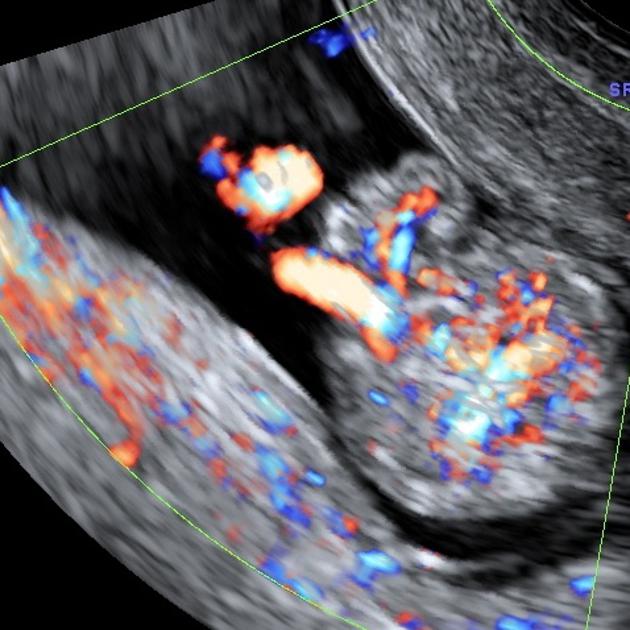
The herniated content is towards the right side of the umbilical cord in most cases; color Doppler may be useful to locate the cord in relation to the herniation. This causes the fetal abdominal circumference to be smaller than expected for gestation age. The herniated bowel often appears free-floating rather than contained. The herniated bowel wall can be thickened due to edema.
There can be either accompanying oligohydramnios or polyhydramnios as ancillary sonographic features.
Treatment and prognosis
There can be an intrauterine mortality rate of 10-15%. The condition of the bowel at birth is the single most important prognostic factor. Some state that the smaller the gastroschisis, the greater the risk of ischemia to the herniated gut due to a more severe restriction of blood flow. Antenatal diagnosis of accompanying fetal bowel dilatation (especially if over 20 mm 8) is also considered a poorer outcome. Liver herniation has been reported in up to 6% of patients, conferring a poor prognostic indicator; 43% survival with herniation versus 97% without 11.
Antenatal diagnosis of gastroschisis may facilitate a planned delivery in a specialized unit (tertiary care center) with parental counseling as well as surgical planning. Most infants are treated surgically on the first day of life. In general, it carries a good survival rate of post-surgery 3.
Complications
There are a number of complications which can mainly involve the bowel and include:
peritonitis: meconium peritonitis
motility dysfunction
fistula formation
neonatal gastro-esophageal reflux: especially following repair 4
History and etymology
The name arises from the Greek "gas-tros'ki-sis", with "gastro" meaning "stomach" and "schisis" meaning "fissure".
Differential diagnosis
General imaging differential considerations include:
omphalocele (particularly if ruptured): is accompanied by a surrounding membrane, cord insertion is central
physiological gut herniation: can occur in early gestation (before 11 weeks)







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.