
In pediatric imaging, the anteroposterior supine chest x-ray is beneficial for imaging unconscious or uncooperative patients.
On this page:
Indications
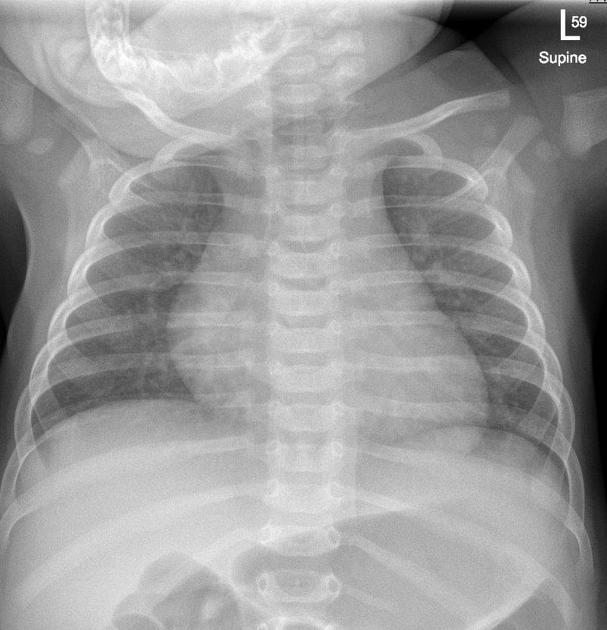
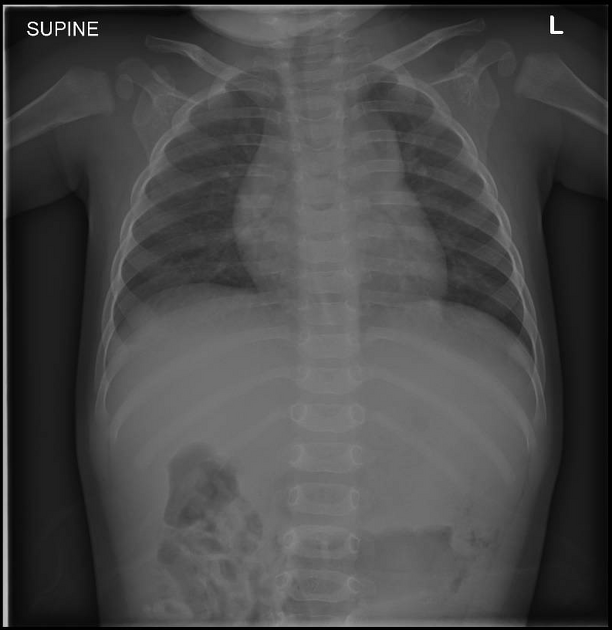
This view is preferred in infant and neonate imaging, whilst AP erect and PA erect views are ideal for children able to cooperate in sitting or standing 1.
As radiation protection is necessary for pediatric patients, it is essential to image the chest properly and avoid unnecessary repeats. If the pediatric patient can only manage a supine view, this is more ideal than performing a poor erect view.
Patient position
- patient is supine
- detector is placed underneath the patient, or the patient is placed on top of the detector
- head is straight and chin ideally out of the field of view
- arms are placed above the patient's head 2
Technical factors
- anteroposterior projection
-
suspended inspiration
- observe breathing by watching the patient's stomach
-
centering point
- the level of the 7th thoracic vertebra; on or above the level of the nipple
- a 10° caudal angle can be used to degrees the patient’s lordosis
-
collimation 3
- superior to the 3rd cervical vertebrae
- inferior to the thoracolumbar junction
- lateral to the skin margins
- it is advised not to collimate too tightly at the apices as breathing may cause the apices to move superiorly
-
orientation
- portrait
-
detector size
- 24 cm x 30 cm or 35 cm x 43 cm depending on the patient’s size
-
exposure 4
- 55-65 kVp
- 1-2 mAs
-
SID
- 110 cm
-
grid
- no
Image technical evaluation
- entire lung fields should be visible; post-processing collimation is not advisable in pediatric imaging (if it is exposed it should be examined). This is particularly important if the clinical indications query a foreign body as demonstrating the abdomen will also be useful in diagnosis
- 6 anterior ribs must be visible to ensure full inspiration
Rotation 5
- the clavicles lie on the same horizontal plane
- measuring the medial ends of the clavicle to the spinous process is not advised due to ossification centers and superior positioning of the shoulder girdle 6
- measure the distances from the 4th ribs lateral border to the center of the spine (upper)
- measure the distances from the 8th ribs lateral border to the center of the spine (lower)
Lead shielding
Contact lead shielding is no longer recommended for any pediatric examination, multiple radiological societies have released statements supporting the cessation of this practice 8-11 the most comprehensive guidance statement on this matter (86 pages) is a joint report found at this citation 12.
Please see your local department protocols for further clarification as they may differ from these recommendations.
Practical Points
In order to streamline workflow, preparing the room beforehand (set up the detector and prepare lead gowns) will be extremely useful in pediatric chest imaging. Placing a pillowcase over the detector will also increase patient comfort.
Ensuring appropriate inspiration and no motion may also require specialized communication techniques to gain cooperation from the child. Examples include:
- “you have to breathe in like you are about to blow out a birthday candle!”
- “take a big sniff now”
- “lets play dead fish!”
- “freeze!”
Immobilization
Some children will maintain their position for the examination, others will not. Research regarding the most effective method of immobilization is lacking. Immobilization methods will range from radiographers holding the child to the utilization of multiple Velcro straps, some departments may consider the latter 'restraint' it is important to clarify with local guidelines.
Family members may assist in distracting or holding the child. It is important to give the parents a focused task; particularly when they are feeling anxious for their children. It is suggested to avoid physical holding due to the scattered radiation given to the parent or holder 7.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.