
A perforated appendix is one of the complications of acute appendicitis. When appendicitis is left untreated, necrosis (gangrene) of the appendiceal wall can occur and progress to a focal rupture.
On this page:
Epidemiology
The rate of perforated appendix varies from 16% to 40%, with a higher incidence in a younger age group and in patients older than 50 years 9. Perforation can be due to a late and atypical presentation of appendicitis, a delay in diagnosis, a delayed decision for surgery, and age-specific physiological changes 1.
Clinical presentation
A slight majority of patients with a perforated appendicitis present more than 48 hours after symptom onset 4.
Pathology
Intraoperative or gross pathology examination reveals a full-thickness defect in the appendiceal wall. Histopathology demonstrates neutrophilic infiltration and transmural necrosis with extensive mucosal ulceration (gangrenous acute appendicitis).
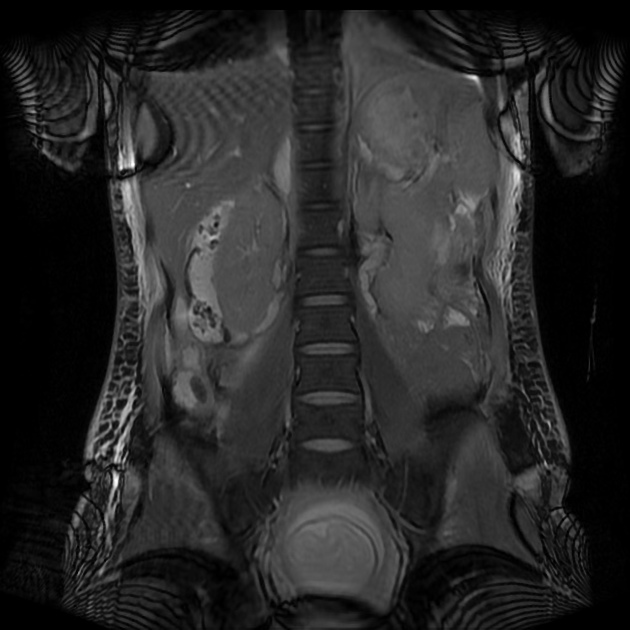
Radiographic features
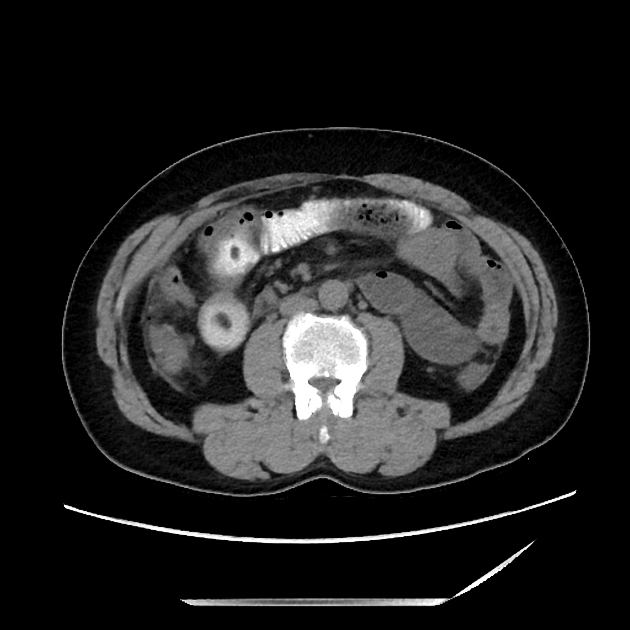
CT
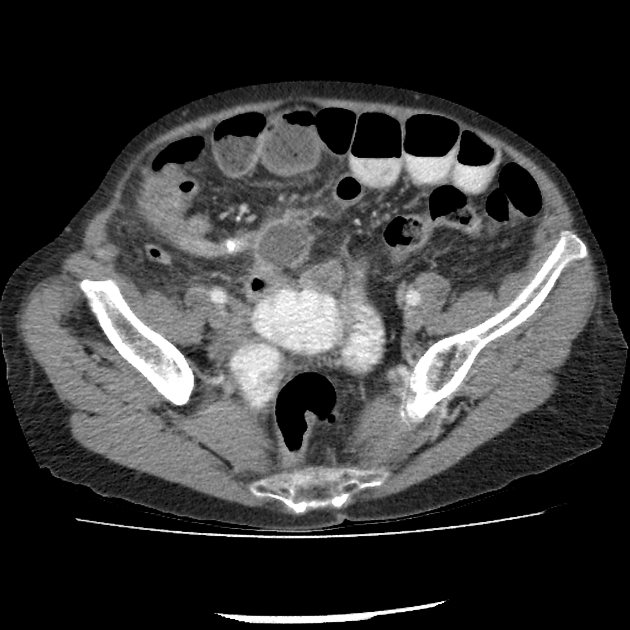
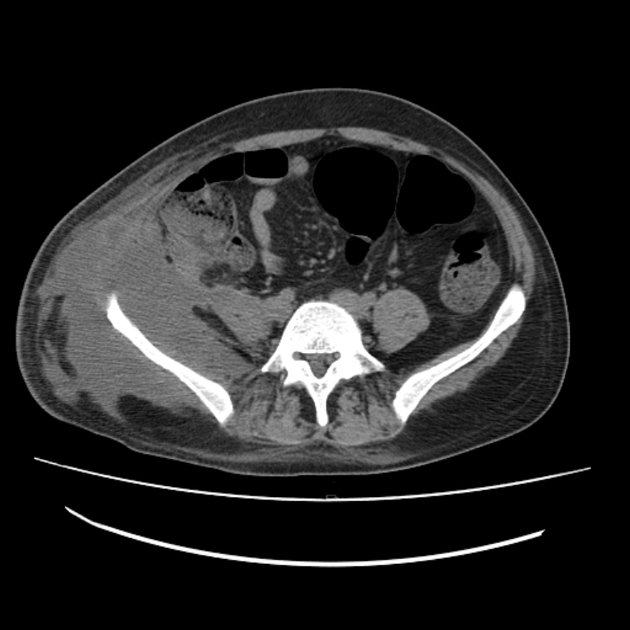
Computed tomography can predict perforation with high specificity (95%) in patients with known appendicitis when certain findings are present 2-6:
focal defect in the enhancing appendiceal wall (most sensitive finding but its performance is heterogeneous across studies 7)
appendicular abscess (most specific finding 10)
extraluminal gas (contained locules or free intraperitoneal gas)
extraluminal appendicolith
extraluminal leak of enteric contrast
Less specific findings include 7:
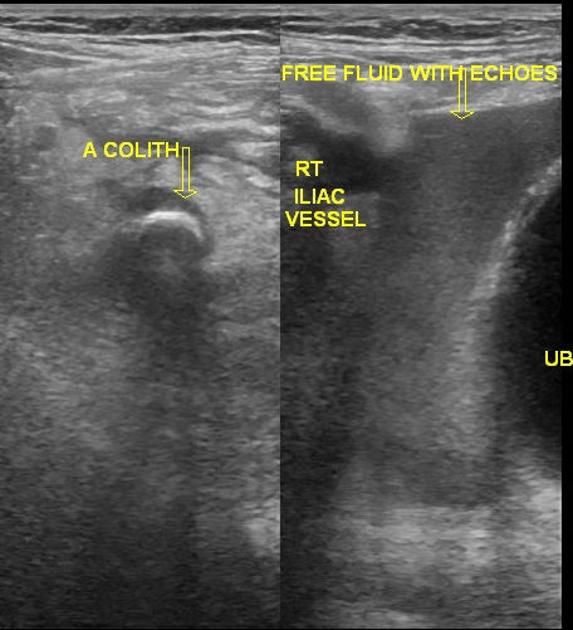
Ultrasound
Although ultrasound is less accurate than a contrast-enhanced CT, the findings can be appreciated in experienced hands. Diagnosis of a perforated appendix relies mainly on demonstration of right iliac fossa abscess or phlegmon in association with signs of appendiceal inflammation and appendicolith.
Treatment and prognosis
Management of perforated acute appendicitis depends on the clinical stability of the patient and the presence of an abscess. A perforated appendix increases the risk of a postoperative abscess. If the patient is unstable or septic, urgent surgery is indicated. If the patient is stable, however, initial nonoperative management including antibiotics is safe 8. If an abscess is present, imaging-guided percutaneous drainage is prudent. Appendectomy should eventually be performed (unless comorbidities contraindicate elective surgery) to exclude an appendiceal neoplasm and prevent recurrent appendicitis.
Differential diagnosis
terminal ileitis with abscess formation (e.g. Crohn disease)
perforated cecal and appendiceal carcinoma










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.