
Rosai-Dorfman disease, also known as sinus histiocytosis with massive lymphadenopathy or Rosai-Dorfman-Destombes disease, is a rare benign idiopathic proliferative disease that involves phagocytic histiocytes.
On this page:
Epidemiology
The disease predominantly occurs in young adults with a mean age at presentation of 21 years. There may be a slight male predominance 7.
Clinical presentation
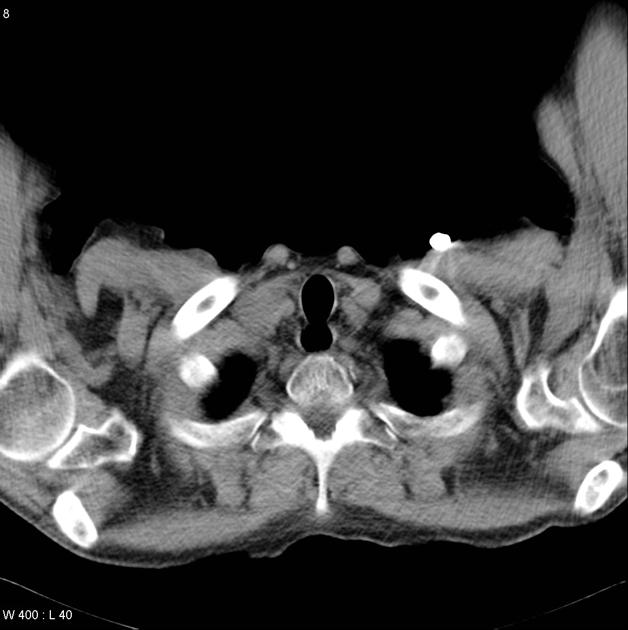
A vast majority of patients (~80%) present with painless massive cervical lymphadenopathy, with associated fever, malaise, weight loss, and night sweats 14.
In individuals with intracranial involvement, headaches and seizures have been described and in many, no systemic manifestations are present 8,14. Additional site-specific signs and symptoms may also be present (e.g. pituitary dysfunction).
Pathology
Etiology
The exact cause of sporadic Rosai-Dorfman disease is unknown but disordered immune regulation and viral infections (e.g. EBV, HHV) are thought to be involved 9.
Familial Rosai-Dorfman disease is due to mutations in SLC29A3.
Location
There is very wide distribution. The condition can affect a multitude of organ systems which include:
-
nodal involvement
cervical lymph nodes (commonest)
mediastinal nodes
-
extranodal involvement (~30% 9)
lungs (~2.5%): nodules and perilymphatic interstitial thickening 9
skin
nasal cavity
orbit: ~7%
bone
kidneys
-
intracranial and spinal disease: rare
dural infiltration is most common (hypertrophic pachymeningitis)
parenchymal involvement is rare
breast (extremely rare)
Microscopic appearance
Histologically, it is characterized by an attenuated infiltration of lymphoplasmacytic cells and histiocytes of varying sizes. The large, pale histiocytic cells contain what looks like engulfed lymphocytes ("emperipolesis") within their cellular borders 14.
Immunophenotype
S100: positive
CD11c: positive
CD68: positive
L1 antigen: positive
CD1a: negative
Radiographic features
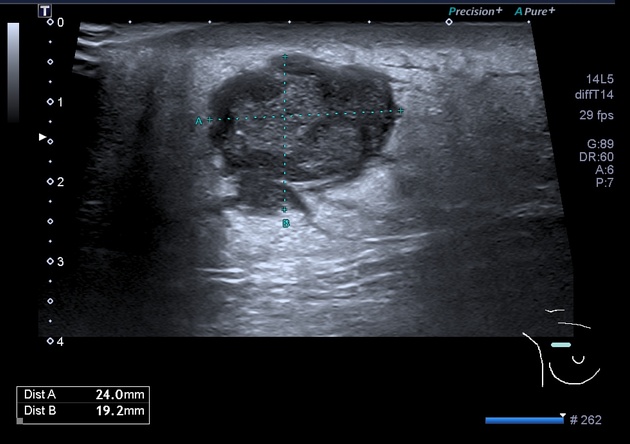
Due to the wide disease spectrum, radiographic features can be variable. Nodal involvement is appreciated as lymphadenopathy on plain film and cross-sectional imaging.
CT
-
central nervous system 8
hyperattenuating meningeal-based mass showing contrast enhancement
parenchymal edema surrounding the lesion may be present
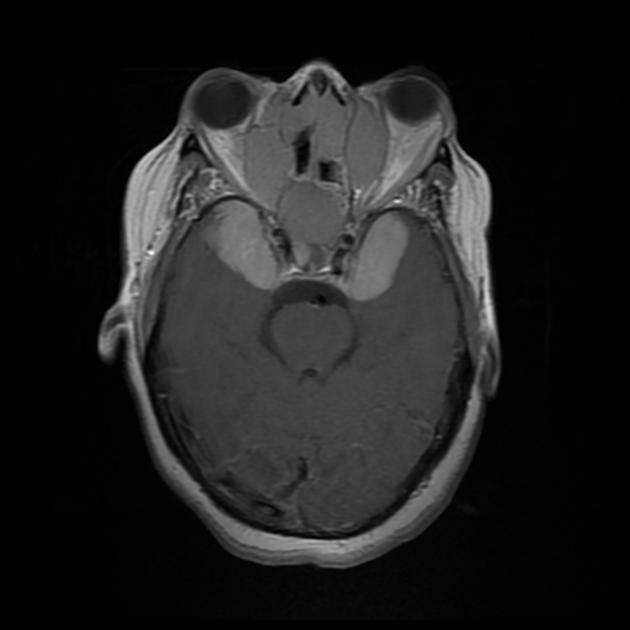
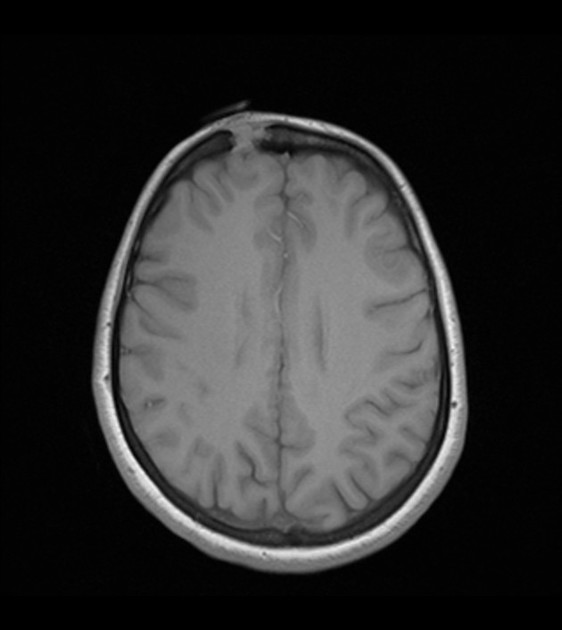
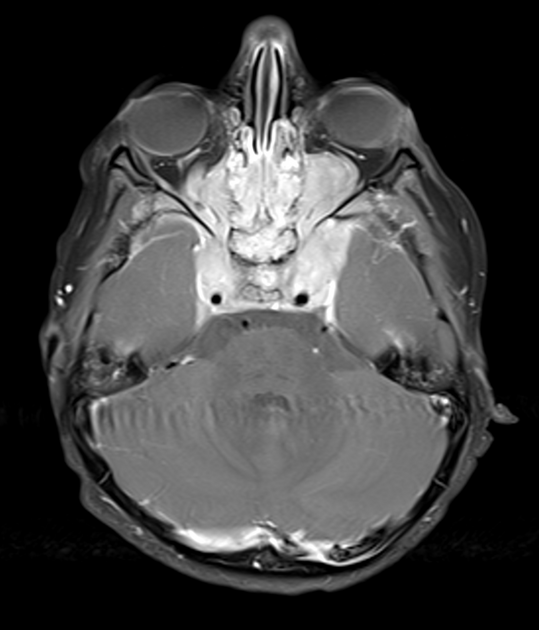
MRI
-
central nervous system 8,14
-
meningeal-based masses
T1: isointense to grey matter
T2: hypointense to grey matter
T1 C+ (Gd): homogeneous enhancement
-
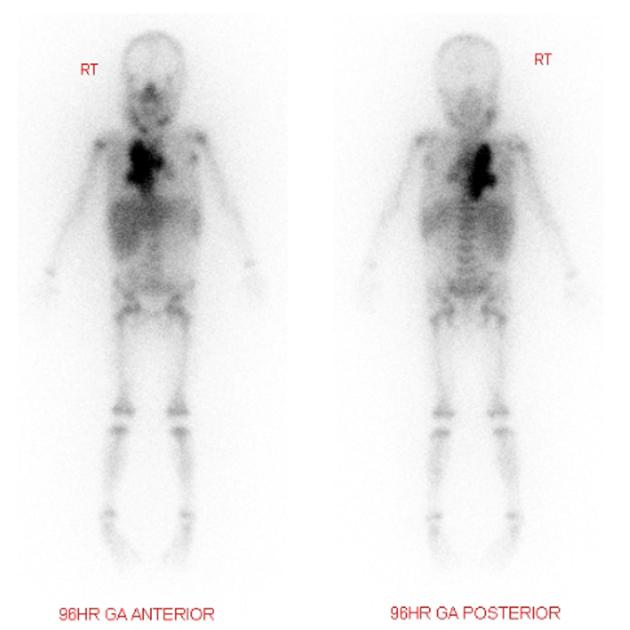
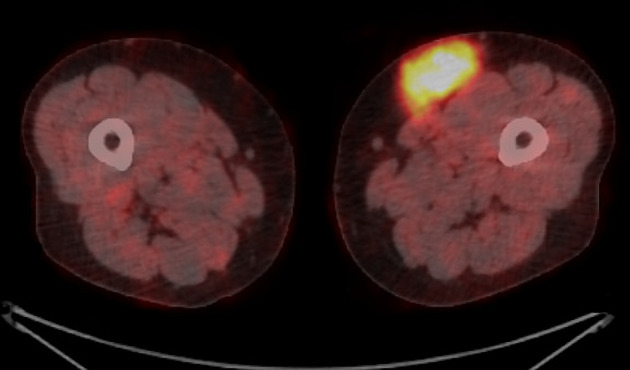
Nuclear medicine
Often shows increased uptake with gallium scanning and increased metabolism with FDG-PET.
Treatment and prognosis
Rosai-Dorfman disease usually follows a benign and self-limiting course with treatment largely targeted at controlling local manifestations (surgical intervention) 6.
History and etymology
This condition was initially described by Juan Rosai (1940-2020) 16 and Ronald F Dorfman (1923-2012) 15 in 1969 3.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}