
High-grade astrocytoma with piloid features (HGAP) is a rare tumor most commonly encountered in the posterior fossa of adults, especially those with neurofibromatosis type 1. It appears heterogeneous and has a relatively poor prognosis.
On this page:
Epidemiology
Due to the small number of patients reported, it is difficult to make strong pronouncements on the epidemiology of this tumor; however, cases so far appear to be primarily in middle-aged and elderly individuals 1,3,4. Neurofibromatosis type 1 appears to be a fairly strong association 1,4.
Pathology
This rare tumor was first included in the 5th Edition (2021) of the WHO classification of CNS tumors as a circumscribed astrocytic glioma 2.
As imaging and histological features are heterogeneous, it is defined by a characteristic DNA-methylation profile 1,4. These tumors can arise both from pre-existing pilocytic astrocytomas or de novo 4.
Location
Although these tumors have been identified in the brain and spinal cord, they have a strong predilection for the posterior fossa (74%), particularly the cerebellum 1,4. NF1-associated HGAPs appear to have a predilection for the midline, including the thalami 4.
Microscopic appearance
The histological appearance of these tumors is varied with reported cases having histological appearances of anaplastic pilocytic astrocytoma or glioblastoma 1. They tend to have elevated mitotic activity, Rosenthal fibers, eosinophilic granular bodies and piloid features (elongated glial tumor cell processes) 4.
Molecular characteristics
Alterations are commonly encountered in 1,4:
Radiographic features
HGAP have heterogenous imaging features, difficult to distinguish from glioblastoma or diffuse midline glioma 4.
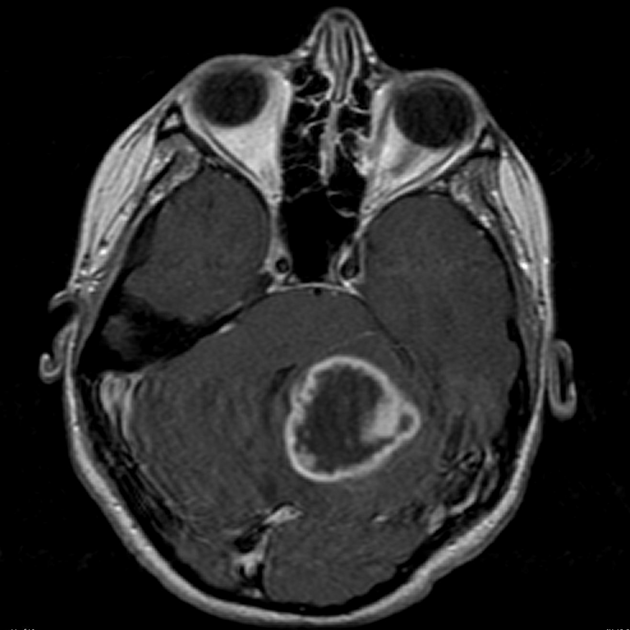
MRI
Due to the small number of cases reported to date, specific or even suggestive imaging features are not yet evident especially as the tumors that have been described are heterogeneous in location (see above) and appearance 1,4.
Generally, they appear to be heterogeneously/peripherally enhancing lesions with low T1 and high T2/FLAIR signal but usually without diffusion restriction of either central or peripheral components 1,4. Cystic areas, necrosis and elevated perfusion have been reported 4.
In the spinal cord they are intramedullary tumors, often with exophytic components and tend to involve the dorsal cord over a long-segment (more than 3 vertebral bodies) 4.
Intraventricular and leptomeningeal dissemination have also been reported 4.
Treatment and prognosis
No tumor specific treatments are available at this time with treatment being empirical consisting of maximal safe surgical resection with concurrent chemoradiotherapy (e.g. temozolomide) 1. There is a suggestion that NF1-associated HGAP may respond mTOR and MAPK inhibitors 4.
Prognosis is poor with a 5-year survival of approximately 50%, somewhat better than glioblastoma IDH-wildtype but worse than IDH-mutant gliomas (astrocytomas and oligodendrogliomas) 1,4.
Differential diagnosis
Due to their heterogeneous appearances and lack of distinctive imaging features, the differential is fairly wide. The diagnosis should be advanced particularly in patients with known NF1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.