
Superficial siderosis of the central nervous system
Updates to Article Attributes
Superficial siderosis of the central nervous system refers to a condition resulting from deposition of haemosiderin along the leptomeninges and subpial surfaces with eventual neurological dysfunction, presumably due to a source of slow and chronic/recurrent subarachnoid bleeding.
Terminology
Superficial siderosis of the central nervous system is a largely infratentorial pathology, and should not be confused with cortical superficial siderosis, which is a supratentorial pathology and has a different aetiopathogenesis with different clinicoradiological stigmata.
Epidemiology
As there are many causes of recurrent or extensive subarachnoid haemorrhage, the demographics are ill-defined and represent those of the underlying cause 1,2. Cases have been reported in patients from a wide range of age groups, including from adolescence to older adults13. Overall, there is a male predilection (M:F 3:1)13.
Clinical presentation
The most common clinical features are 1-3:
-
progressive and bilateral
-
cerebellar ataxia
often prominent gait ataxia
pyramidal and other long-tract signs
Less common clinical features include 1-3:
myelopathy (e.g. neurogenic bladder)
cognitive impairment
hyposmia or anosmia
seizures
clinical features of spontaneous intracranial hypotension may also be present depending on the cause 4,5
If cerebrospinal fluid samples are taken via lumbar puncture, red blood cells and/or xanthochromia is commonly present 2.
Pathology
Superficial siderosis of the central nervous system is thought to result from recurrent occult subarachnoid bleeds from spinal dural pathologies, although the source of bleeding is not usually identified on imaging 1,2. Although it is common to see a small amount of haemosiderin deposition at the margins of a previous haemorrhage or surgical resection margin, a single episode of subarachnoid haemorrhage (e.g. berry aneurysm rupture) is usually not sufficient to result in this condition 1,2.
Most patients will have a history of either spinal trauma (especially with ventral dural tears) or previous intradural neurosurgical intervention, and it is thought that these result in friable vessels prone to causing chronic or recurrent subarachnoid bleeding 2. Rarely, patients will have tumours or vascular malformations as the cause for superficial siderosis of the central nervous system 1,2.
The result of this subarachnoid bleeding, regardless of aetiology, is accumulation of iron and its degradation products in the leptomeninges and subpial structures 1,2. Given these products are neurotoxic, there is subsequent neuronal loss and eventual atrophy of affected regions of the central nervous system 1. The prominent involvement of the vestibulocochlear nerve (CN VIII), which results in sensorineural hearing loss, is believed to be due to the combination of a long cisternal course (thus with ample exposure to the subarachnoid space) and the susceptibility of microglial cells (which have a role in myelination) to be damaged by iron compounds 6.
Aetiology
There are many aetiologies 1-9:
idiopathic
-
spinal dural defects
traumatic cervical nerve root avulsion
dural defect with spinal CSF collections/spinal cyst
postoperative pseudomeningocoele
-
vascular abnormalities
fragile capillary regrowth after neurosurgery
friable vessels due to dural ectasia
-
intracranial neoplasms
occult small ependymoma
Radiographic features
CT
CT brain is often normal, but in some cases, there may be a hyperdense ring appreciated around the brainstem 2.
Angiography (DSA)
Usually unrewarding and will usually not demonstrate a point of bleeding 2.
MRI
Brain
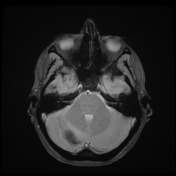
MRI brain is the modality of choice for assessment and diagnosis of superficial siderosis of the central nervous system 1,2. The findings are characteristic, with all pial and ependymal surfaces coated symmetrically with T2/T2* low signal haemosiderin, particularly those of the brainstem and cerebellum (the cerebellar vermis and folia are classic locations for identifying subtle deposits), but can be more extensive to involve the Sylvian fissure and even sulcal convexities 1,2. In long-standing cases, cerebellar atrophy will inevitably develop, particularly affecting the superior vermis 2.
T1: low signal
T2: low signal
GRE/SWI: low signal with blooming
Spinal cord
As part of the workup for superficial siderosis, if no lesion is identified in the intracranial compartment, then imaging of the entire spinal canal should be performed (e.g. superficial siderosis due to myxopapillary ependymoma). In the spinal cord, like in the brain, the pial surfaces are again typically coated with T2/T2* low signal haemosiderin 1,2.
Treatment and prognosis
Workup and management is focused on identifying the causative lesion, although often even this is not possible. Regardless of cause, iron chelating agents may have benefit 10.
When no correctable cause is identified, signs and symptoms are slowly progressive.
History and etymology
Superficial siderosis of the central nervous system was first described by Ralph C Hamill in 1908 11.
Differential diagnosis
-
cortical superficial siderosis
e.g. cerebral amyloid angiopathy can also result in cerebellar superficial siderosis 12
-
cerebellar bleeding following craniectomy, spinal surgery or lumbar puncture
-<p><strong>Superficial siderosis of the central nervous system</strong> refers to a condition resulting from deposition of haemosiderin along the leptomeninges and subpial surfaces with eventual neurological dysfunction, presumably due to a source of slow and chronic/recurrent subarachnoid bleeding.</p><h4>Terminology</h4><p>Superficial siderosis of the central nervous system is a largely infratentorial pathology, and should not be confused with <a href="/articles/cortical-superficial-siderosis" title="cortical superficial siderosis">cortical superficial siderosis</a>, which is a supratentorial pathology and has a different aetiopathogenesis with different clinicoradiological stigmata.</p><h4>Epidemiology</h4><p>As there are many causes of recurrent or extensive subarachnoid haemorrhage, the demographics are ill-defined and represent those of the underlying cause <sup>1,2</sup>. Cases have been reported in patients from a wide range of age groups, including from adolescence to older adults. Overall, there is a male predilection (M:F 3:1).</p><h4>Clinical presentation</h4><p>The most common clinical features are <sup>1-3</sup>:</p><ul>- +<p><strong>Superficial siderosis of the central nervous system</strong> refers to a condition resulting from deposition of haemosiderin along the leptomeninges and subpial surfaces with eventual neurological dysfunction, presumably due to a source of slow and chronic/recurrent <a href="/articles/subarachnoid-haemorrhage" title="Subarachnoid haemorrhage">subarachnoid bleeding</a>.</p><h4>Terminology</h4><p>Superficial siderosis of the central nervous system is a largely infratentorial pathology, and should not be confused with <a href="/articles/cortical-superficial-siderosis" title="cortical superficial siderosis">cortical superficial siderosis</a>, which is a supratentorial pathology and has a different aetiopathogenesis with different clinicoradiological stigmata.</p><h4>Epidemiology</h4><p>As there are many causes of recurrent or extensive subarachnoid haemorrhage, the demographics are ill-defined and represent those of the underlying cause <sup>1,2</sup>. Cases have been reported in patients from a wide range of age groups, including from adolescence to older adults <sup>13</sup>. Overall, there is a male predilection (M:F 3:1) <sup>13</sup>.</p><h4>Clinical presentation</h4><p>The most common clinical features are <sup>1-3</sup>:</p><ul>
-<li><p><a href="/articles/cortical-superficial-siderosis" title="cortical superficial siderosis">cortical superficial siderosis</a></p></li>- +<li>
- +<p><a href="/articles/cortical-superficial-siderosis" title="cortical superficial siderosis">cortical superficial siderosis</a></p>
- +<ul><li><p>e.g. <a href="/articles/cerebral-amyloid-angiopathy-1" title="Cerebral amyloid angiopathy">cerebral amyloid angiopathy</a> can also result in cerebellar superficial siderosis <sup>12</sup></p></li></ul>
- +</li>
References changed:
- 12. Koemans E, Voigt S, Rasing I et al. Cerebellar Superficial Siderosis in Cerebral Amyloid Angiopathy. Stroke. 2022;53(2):552-7. <a href="https://doi.org/10.1161/STROKEAHA.121.035019">doi:10.1161/STROKEAHA.121.035019</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/34538086">Pubmed</a>
- 13. Fearnley J, Stevens J, Rudge P. Superficial Siderosis of the Central Nervous System. Brain. 1995;118 ( Pt 4)(4):1051-66. <a href="https://doi.org/10.1093/brain/118.4.1051">doi:10.1093/brain/118.4.1051</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/7655881">Pubmed</a>
Image 2 MRI (Gradient Echo) ( destroy )
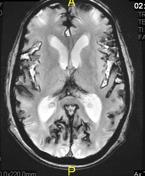
Image 2 MRI (Gradient Echo) ( update )

Image 10 MRI (Gradient Echo) ( create )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.