
Diffuse astrocytoma NOS
Updates to Case Attributes
IDH-1 negative / not mutated/nonmutated is known as IDH wild-type, and carries a worse prognosis than IDH mutated-mutated diffuse gliomas.
-<p>IDH-1 negative / not mutated is known as IDH wild-type, and carries a worse prognosis than IDH mutated diffuse gliomas. </p>- +<p>IDH-1 negative/nonmutated is known as IDH wild-type, and carries a worse prognosis than IDH-mutated diffuse gliomas. </p>
References changed:
- Boots-Sprenger SH, Sijben A, Rijntjes J, Tops BB, Idema AJ, Rivera AL, Bleeker FE, Gijtenbeek AM, Diefes K, Heathcock L, Aldape KD, Jeuken JW, Wesseling P. Significance of complete 1p/19q co-deletion, IDH1 mutation and MGMT promoter methylation in gliomas: use with caution. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 26 (7): 922-9. <a href="https://doi.org/10.1038/modpathol.2012.166">doi:10.1038/modpathol.2012.166</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/23429602">Pubmed</a> <span class="ref_v4"></span>
Updates to Study Attributes
Very large left frontal mass measuring approximately 9.1 x 7.0 x 6.3 cm. It is
has high T2 signal with loss of grey-white differentiation and gyral expansion,
. It appears very heterogeneous ofon FLAIR, studded with numerous small cystic spaces, and has mildly heterogeneous low T1 signal. It
cross crosses the midline via an expanded corpus callosumcallosal genu. There is a smallamount of surrounding high FLAIR signal. No diffusion restriction. Nodefinite enhancement. At the inferolateral aspect of the mass is someintrinsic T1 signal, likely haemorrhage with corresponding susceptibility
artifact artefact and precontrast hyperdensity on the CT. No increased CBV. MRSdemonstrated low NAA and reversal of the normal choline-creatine ratio.
Image MRI (ADC) ( update )
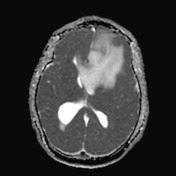
Image 3 MRI (T2) ( update )

Image 4 MRI (DWI) ( update )

Image 5 MRI (ADC) ( update )
Image 6 MRI (SWI) ( update )
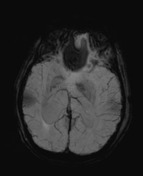
Image 7 MRI (T1 C+) ( update )
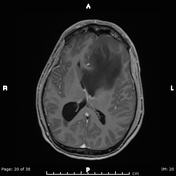
Image 8 MRI (Fused T1C+/CBV) ( update )

Updates to Study Attributes
There is a large low-density intra-axial mass with centred in the left frontal lobe and, crossing the midline via the corpus callosum. Marked compression of the frontal horns of the lateral ventricles, with up to 10 mm of rightward subfalcine midline shift. No enhancement is appreciated.
Updates to Freetext Attributes
The patient proceeded to surgery.
Histopathology
MICROSCOPIC DESCRIPTION: Paraffin sections show a moderately hypercellular glial tumour. The majority of tumour cells have oligodendroglial morphological features with moderately pleomorphic round and oval hyperchromatic nuclei and a paucity of delicate processes. Moderate numbers of mini-gemistocytes and gliofibrillary oligodendroglial cells are also noted. There is prominent microcyst formation. Scattered mitotic figures are noted (2 in 20 HPF). There is no microvascular proliferation and no necrosis is identified. The features are of a diffuse glioma favouring oligodendroglioma (WHO Grade II).
IMMUNOHISTOCHEMISTRY:
- GFAP positive
- Nestin positive (low)
- Nogo A negative
- IDH-1 R132H negative (not mutated)
- ATRX negative (mutated)
- p53 positive
- MGMT negative (likely methylated)
- p16 CDKN2A positive
- Topoisomerase labelling index: Approximately 2%.
DIAGNOSIS: IDH wild type diffuse astrocytoma (WHO Grade II).





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.