
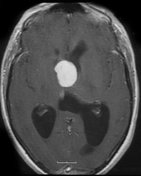
Intraventricular meningioma - third ventricle
Updates to Case Attributes
Although the histology is atypical for meningioma (see below), thehas remained well 5 years after resection without evidence ofwent on to have a systemic malignancyresection.
Histology
Paraffin sections show a densely hypercellular spindle cell tumour. Tumour cells have mildly pleomorphic elongated vesicular nuclei and coarse bipolar processes and are arranged in intersecting fasciculi. A very occasional mitotic figure is identified. No necrosis is seen. No brain parenchymal tissue is included.
Very weak immunostaining for epithelial membrane antigen (EMA) is noted in tumour cells in some areas. Approximately 2-3% of tumour cells show strong nuclear staining for Ki-67. No immunostaining for cytokeratins (AE1/AE3, CAM 5.2; CK 7, CK 20), S-100 protein, GFAP, neurofilament protein, CD34, tyrosinase or smooth muscle actin (SMA) is seen in tumour cells.
Final diagnosis:
Third ventricle tumour: Undifferentiated spindle cell tumour of uncertain malignant potential.
Comment:
Although the regional weak immunostaining for epithelial membrane antigen (EMA) in this tumour is consistent with meningioma, the histological appearances of tumour cells and their architectural arrangement are unusual for meningioma and are more suggestive of a mesenchymal tumour. Metastasis from a low grade sarcoma or gastro-intestinal stromal tumour (GIST) cannot be excluded.
Discussion
Although the histology is unusual for meningioma, the patient has remained well 5 years after resection without evidence of a systemic malignancy.
-<p>Although the histology is atypical for <a href="/articles/meningioma" style="padding-top: 0px; padding-right: 0px; padding-bottom: 0px; padding-left: 0px; margin-top: 0px; margin-right: 0px; margin-bottom: 0px; margin-left: 0px; color: rgb(0, 102, 153); background-image: initial; background-repeat: initial; background-attachment: initial; -webkit-background-clip: initial; -webkit-background-origin: initial; background-color: transparent; text-decoration: none; background-position: initial initial; ">meningioma</a> (see below), the patient has remained well 5 years after resection without evidence of a systemic malignancy.</p><h5>Histology</h5><p>Paraffin sections show a densely hypercellular spindle cell tumour. Tumour cells have mildly pleomorphic elongated vesicular nuclei and coarse bipolar processes and are arranged in intersecting fasciculi. A very occasional mitotic figure is identified. No necrosis is seen. No brain parenchymal tissue is included. Very weak immunostaining for epithelial membrane antigen (EMA) is noted in tumour cells in some areas. Approximately 2-3% of tumour cells show strong nuclear staining for Ki-67. No immunostaining for cytokeratins (AE1/AE3, CAM 5.2; CK 7, CK 20), S-100 protein, GFAP, neurofilament protein, CD34, tyrosinase or smooth muscle actin (SMA) is seen in tumour cells.</p><h5>Final diagnosis:</h5><p>Third ventricle tumour: Undifferentiated spindle cell tumour of uncertain malignant potential.</p><h5>Comment: </h5><p>Although the regional weak immunostaining for epithelial membrane antigen (EMA) in this tumour is consistent with meningioma, the histological appearances of tumour cells and their architectural arrangement are unusual for meningioma and are more suggestive of a mesenchymal tumour. Metastasis from a low grade sarcoma or gastro-intestinal stromal tumour (GIST) cannot be excluded.</p>- +<p>The patient went on to have a resection. </p><p><strong>Histology</strong></p><p>Paraffin sections show a densely hypercellular spindle cell tumour. Tumour cells have mildly pleomorphic elongated vesicular nuclei and coarse bipolar processes and are arranged in intersecting fasciculi. A very occasional mitotic figure is identified. No necrosis is seen. No brain parenchymal tissue is included.</p><p>Very weak immunostaining for epithelial membrane antigen (EMA) is noted in tumour cells in some areas. Approximately 2-3% of tumour cells show strong nuclear staining for Ki-67. No immunostaining for cytokeratins (AE1/AE3, CAM 5.2; CK 7, CK 20), S-100 protein, GFAP, neurofilament protein, CD34, tyrosinase or smooth muscle actin (SMA) is seen in tumour cells.</p><p><em>Final diagnosis:</em></p><p>Third ventricle tumour: Undifferentiated spindle cell tumour of uncertain malignant potential.</p><p><em>Comment:</em> </p><p>Although the regional weak immunostaining for epithelial membrane antigen (EMA) in this tumour is consistent with meningioma, the histological appearances of tumour cells and their architectural arrangement are unusual for meningioma and are more suggestive of a mesenchymal tumour. Metastasis from a low grade sarcoma or gastro-intestinal stromal tumour (GIST) cannot be excluded.</p><p><strong>Discussion</strong></p><p>Although the histology is unusual for meningioma, the patient has remained well 5 years after resection without evidence of a systemic malignancy. </p>
Updates to Study Attributes
Intraventricular meningioma
No other subependymal nodules or calcifications identified to suggest tuberous sclerosis.
Image MRI (T1 C+) ( update )
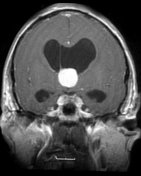
Image MRI (T1 C+) ( update )
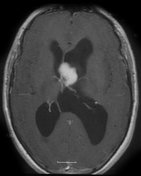
Image MRI (T1 C+) ( update )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.