

1/It’s rare that a patient can tell exactly you where their pathology is—but that’s what they’re doing when they have a cranial nerve palsy—you just have to know where to look!
A thread about Six Syndromes of the Sixth Cranial Nerve. If you know the syndrome, you know the answer!


2/To understand the six syndromes, you must know the anatomy of the 6th nerve. It starts in the brainstem, at the facial colliculus—what looks like the cute baby butt of the brainstem. It then travels anteriorly through the brainstem to exit out the ventral surface of the pons.
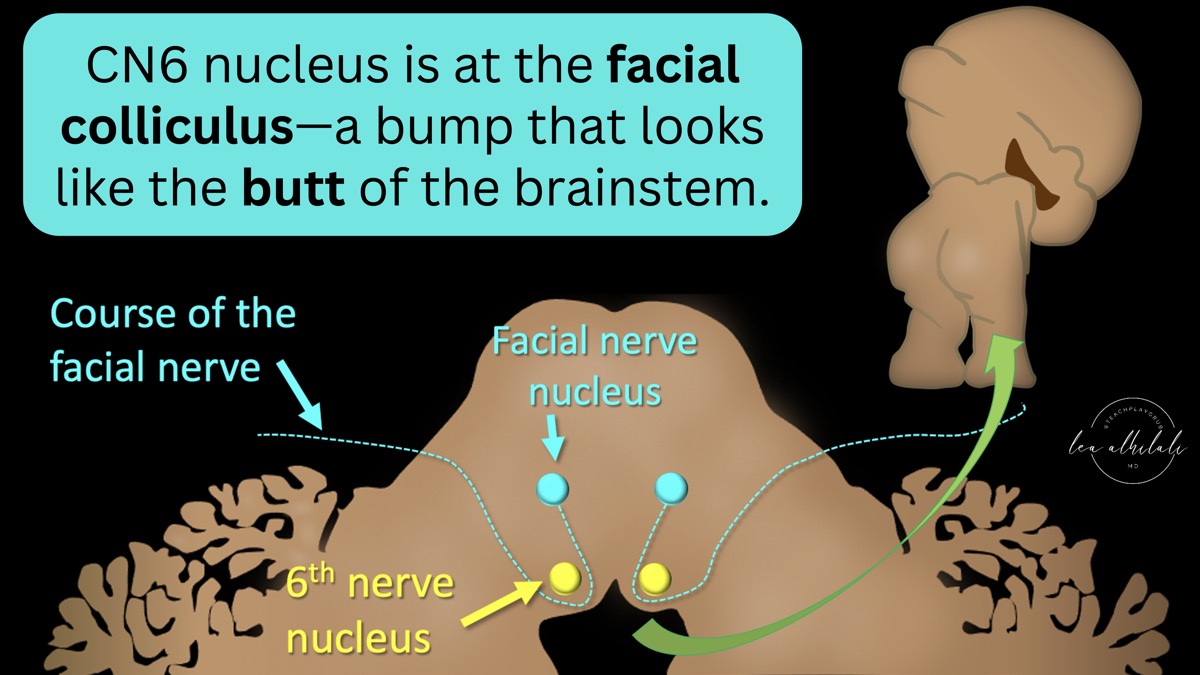
3/It exits the brainstem at the inferior aspect of the pons—under what looks like pot belly of the pons, what I call the “dad bod” of the pons and then travels anteriorly in the subarachnoid space towards the clivus. Think of it like the belt under the pot belly

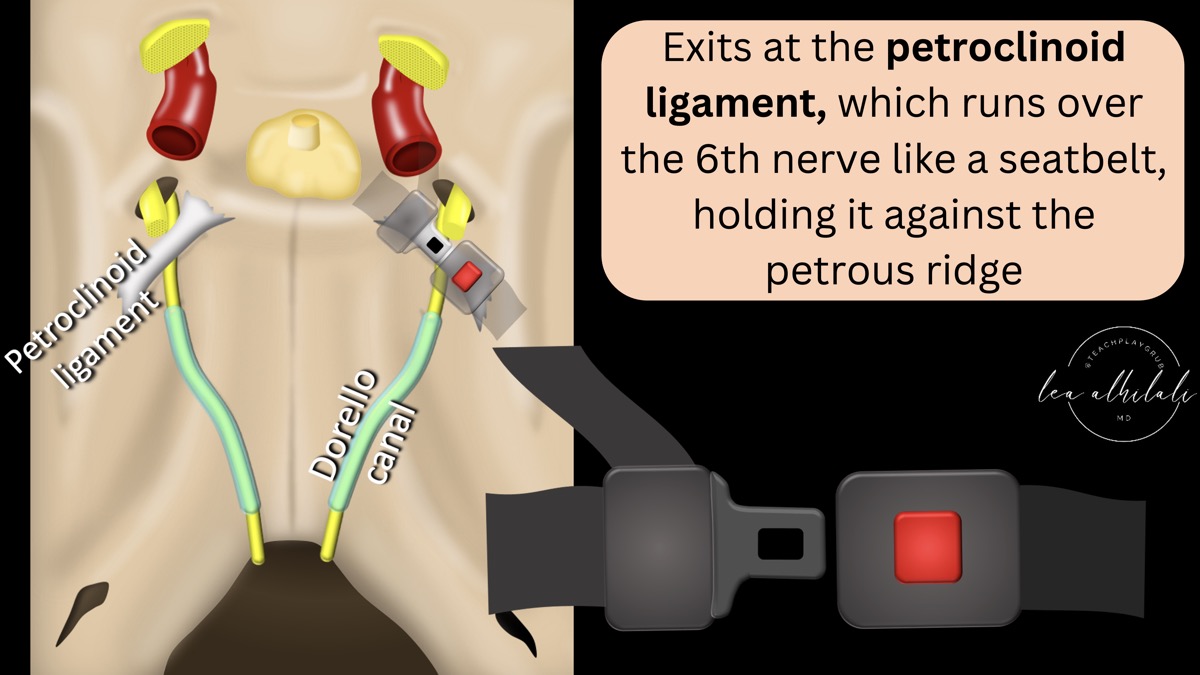
4/It then enters Dorello canal, a channel that I think sounds more like a canal in Venice than anatomic structure. This channel is at the lateral aspect of the posterior clivus & travels superiorly—taking the nerve up towards the orbit, where it needs to go to innervate the lateral rectus muscle

5/The exit of Dorello canal is marked by the petroclinoid ligament. Which, as its name implies, runs between the petrous ridge and clinoid. The 6th nerve runs under this ligament, which holds it down against the medial petrous ridge like a seatbelt.
6/It then enters the cavernous sinus, where cranial nerves 3, 4, and 5, as well as the ICA and sympathetics also run. It is located more medially than the other nerves—in fact, it is the only nerve to run in the cavernous sinus itself, rather than in the wall.

7/It’s like the sixth nerve is sitting in the cavernous sinus VIP section & all the other nerves have to stay outside the velvet rope—in the wall of the sinus

8/It exits the cavernous sinus to enter the orbit through the superior orbital fissure. Here, it is joined by CN 3 and 5, with CN 2 in close proximity. As soon as it enters the orbit, it makes an immediate turn laterally and innervates the lateral rectus muscle.

9/Its orbital course is like your course when you realize you’ve almost missed your exit on the highway—so you take the sharpest possible turn lateral to be able to make your exit

10/Here’s a recap of the course of the 6th nerve. Remember it—b/c where the pathology is along the nerve course determines which syndrome we see! At each point of the course, injury to the nerve causes a different syndrome—giving us the 6 syndromes of the 6th cranial nerve!

11/There are six syndromes of the cranial nerve—one for each of its five stops along the way to its destination in the orbit—and one that is idiopathic

12/The syndrome we get depends on the location of the lesion. Here are the syndromes laid out against the region of the cranial nerve course they are associated with

13/In the brainstem, many important structures are near the 6th nerve nucleus & its course through the brainstem as it exits. Notably, pyramidal tracts containing your motor fibers are in direct proximity with the intraaxial 6th nerve.
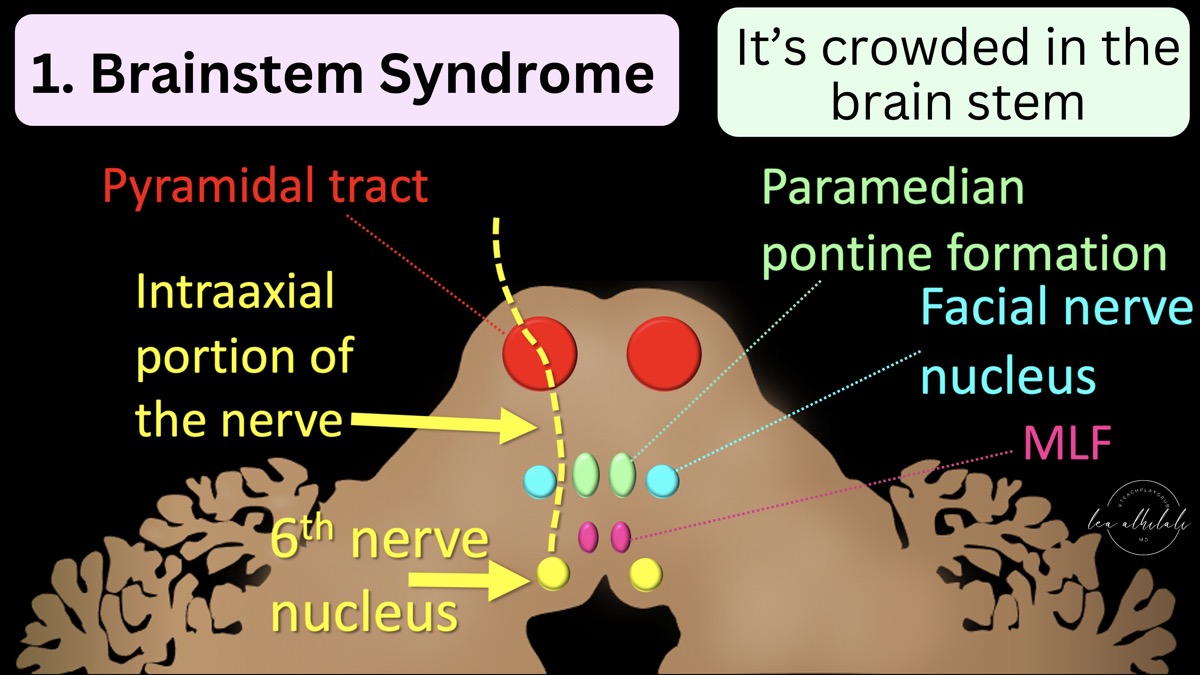
14/Compressive, ischemic or inflammatory lesions may affect CN 6 here, but likely other CNs & the pyramids will be affected. There are specific syndromes, but the key point is there will be other deficits. And MOTOR/WEAKNESS is a deficit unique to a brainstem lesion!

15/Structures in the brainstem are crowded. So injury here is like having an explosion in a crowded city, you aren’t just going to hit one person. So brainstem lesions are unlikely to be isolated

16/In the subarachnoid space & Dorello canal, CN6 is susceptible to changes in intracranial pressure. B/c CN6 is tethered in Dorello canal, when the brainstem moves w/changes in pressure, it is stretched. Therefore changes in intracranial pressure can uniquely give you bilateral isolated CN6 palsies!

17/The CSF space is like a balloon. Unlike any other cranial nerve, CN runs along the outside of the balloon in Dorello canal. Increased intracranial pressure is like over distending the balloon

18/This overinflated balloon presses on CN6 along its outside. Unfortunately for CN6, the clivus is on the other side, so it gets compressed like a sandwich between the overinflated CSF balloon and the clivus.

19/As it exits Dorello canal & travels under the petroclinoid ligament, complicated otitis media w/petrous apicitis can affect it. Isolated palsies are rare here b/c adjacent nerves, especially CN8. So if they have a complex palsy w/hearing symptoms—think of this region!

20/After it enters the cavernous sinus, things start to get complicated. B/c of all the nerves in close proximity, isolated palsies are rare here. Cavernous sinus syndrome is deficits of two or more of these structures. Both the deficits & differential diagnosis are extensive.

21/Pathology invading the cavernous sinus is like a bulldozer plowing through the club. It’s going to hit everyone & won’t respect the velvet rope separating CN6 from the other nerves. So again—an isolated palsy is rare

22/It then enters the orbit. It has a short orbital course—immediately taking a lateral turn after the SOF to innervate the lateral rectus. So not much of CN6 is separated from other nerves, & lesions here will cause a SOF syndrome or orbital apex syndrome, not an isolated palsy

23/It’s like a highway—most of the accidents are going to be on the big crowded main road (the orbital apex) and not the tiny, short off ramp (tiny intraorbital course).

24/The last syndrome isn’t anatomic. It’s when there is no other identifiable cause—the transverse myelitis of CN6! (likely microvascular/post-inflammatory). One quarter of CN6 palsies are idiopathic. But you must rule out the other 5 syndromes before calling this!

25/Now you know the Six Syndromes of the Sixth Cranial Nerve. It’s only isolated in the subarachnoid space & Dorello. Otherwise, associated deficits help localize. Now go impress a neurologist!
See this & other great exhibits at: radiopaedia.org/courses/rposter






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.