
Odontogenic keratocysts (OKC), previously known as keratocystic odontogenic tumors (KCOT or KOT), are rare benign cystic lesions involving the mandible or maxilla and are believed to arise from dental lamina. Whether these lesions are developmental or neoplastic is controversial, with the 4th edition (2017) WHO classification placing it back into the developmental lesion category. They are locally aggressive and tend to recur after excision.
On imaging, they typically appear as an expansile solitary unilocular lesion extending longitudinally in the posterior portions of the mandible. Although the majority are solitary, in 5-10% of cases multiple odontogenic keratocysts will be present: an associated condition such as basal cell nevus syndrome should be considered in these cases.
On this page:
Epidemiology
Odontogenic keratocysts predominantly occur in younger patients (2nd to 3rd decades) 1,7 and may be seen in either the body or ramus of the mandible (~70% of all odontogenic keratocysts) or maxilla, comprising 5-10% of all jaw cysts. There may be a male predilection.
Associations
-
basal cell nevus syndrome (or Gorlin-Goltz syndrome)
strong association
consider the diagnosis if multiple odontogenic keratocysts are present
Clinical presentation
Commonly discovered incidentally. When symptomatic, jaw swelling and pain are common symptoms associated with these tumors 8. Less commonly, trismus and paresthesia may occur.
Pathology
Gross specimen examination reveals a thin-walled, friable cyst containing fluid and debris. Viscosity of the contents ranges from straw-colored fluid to purulent and cheese-like masses.
They originate from epithelial cell rests (stratified squamous keratinizing epithelium) found along the dental lamina and periodontal margin of the alveolus of the mandible 7. Inflammation may impede histologic characterization.
Radiographic features
Plain radiograph
OPG
They are typically seen as a solitary, radiolucent, unilocular, expansile lesion with smooth, corticated borders 5. These cortices are often scalloped around the roots of teeth. Three-quarters of lesions are located in the posterior mandible. When in the mandible, they typically grow along the length of the bone with minimal buccolingual expansion. In the maxilla, they expand into the maxillary sinus.
The appearance and location can vary 10. If associated with the crown of an unerupted/impacted tooth, they can mimic a dentigerous cyst. If associated with the roots of a non-vital tooth, they can mimic a radicular cyst. If large enough, they will resorb the roots of adjacent teeth. They may occasionally appear septated, making the distinction from ameloblastoma difficult.
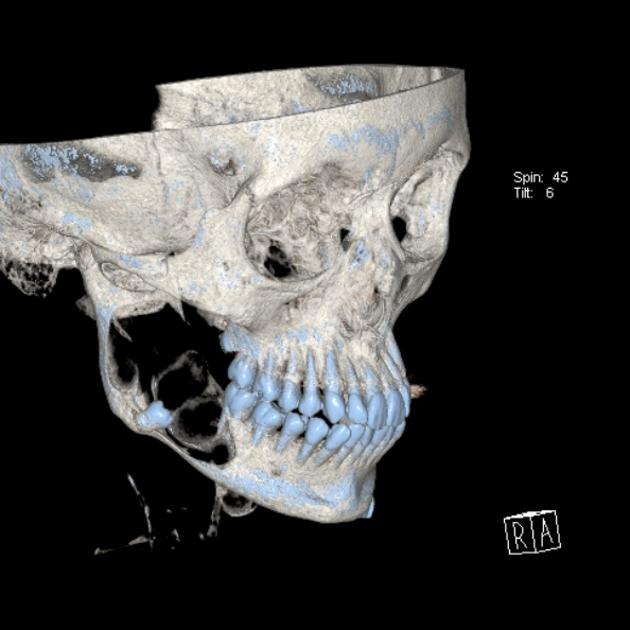
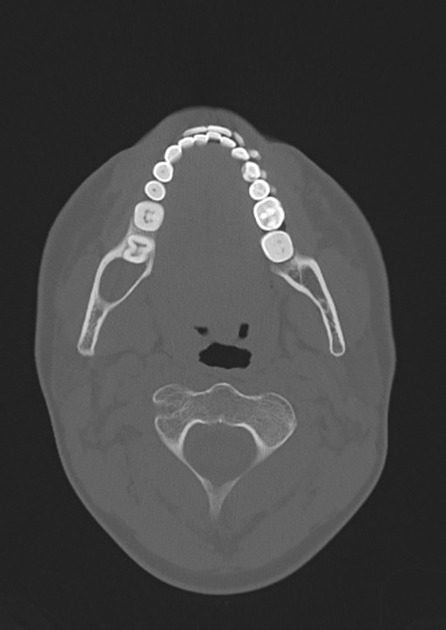
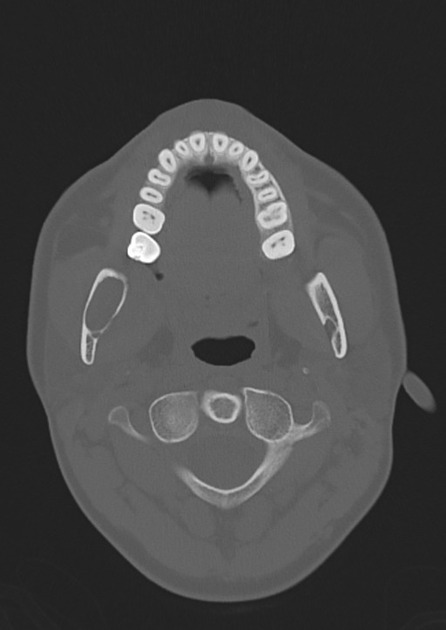
CT
Reminiscent of plain radiographic findings, but in better detail. Visualized as an expansile, cystic lesion with scalloped, well-corticated borders. Density of cystic contents varies with viscosity. Cortical breach suggests possible soft tissue involvement.
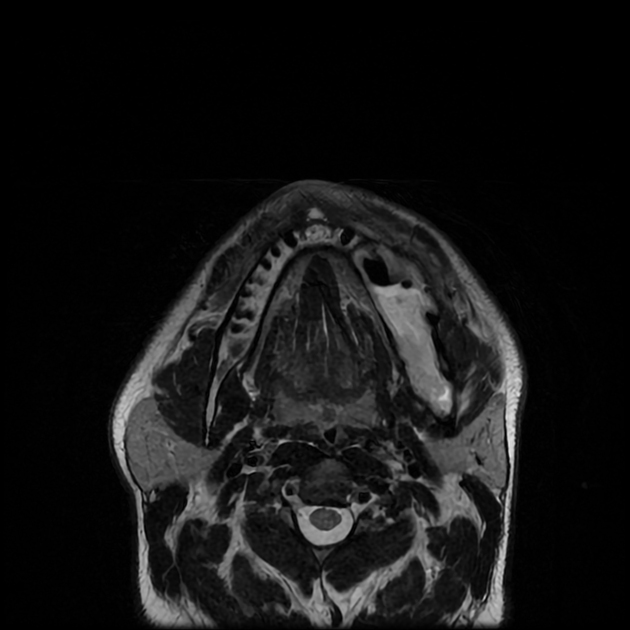
MRI
Odontogenic keratocysts will typically demonstrate 3:
T1: high signal due to cholesterol and keratin contents
T2: heterogeneous signal
DWI/ADC: restricts due to presence of keratin
-
T1 C+ (Gd)
peripheral enhancement
no enhancing nodular component (unlike ameloblastomas)
Treatment and prognosis
They are locally aggressive. Treatment is often with marsupialization/enucleation/excision +/- aggressive curettage. However, they can have a very high recurrence rate (30-60%), and follow-up is essential.
History and etymology
It was first described by H P Philipsen in 1956 as an odontogenic keratocyst.
Differential diagnosis
Imaging differential considerations include:
-
both dentigerous cysts and odontogenic keratocysts can be positioned pericoronally
dentigerous cysts tend to attach at the cemento-enamel junction of teeth
-
does not scallop, does not exhibit septation, and is often more expansile
radicular cysts are centered at the apices of non-vital teeth
-
tend to be multilocular, more expansile, with a textbook soap-bubble or honeycomb appearance
tendency for ameloblastoma to be more aggressive and cause more significant tooth resorption
long-standing odontogenic keratocyst may mimic ameloblastoma
ameloblastic fibroma: in younger individuals, if the lesion is pericoronal to an impacted tooth
-
simple bone cyst in younger individuals
can be challenging to differentiate, but usually simple bone cysts exhibit minimal expansion, and spare the lamina dura as well as the periodontal ligament spaces
odontogenic keratocysts will tend to efface the lamina dura
















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}